Case No.: A-010
Diagnosis: Pseudomembranous colitis
Organ: Colon
Last Updated: 3/21/2011
|
|
|
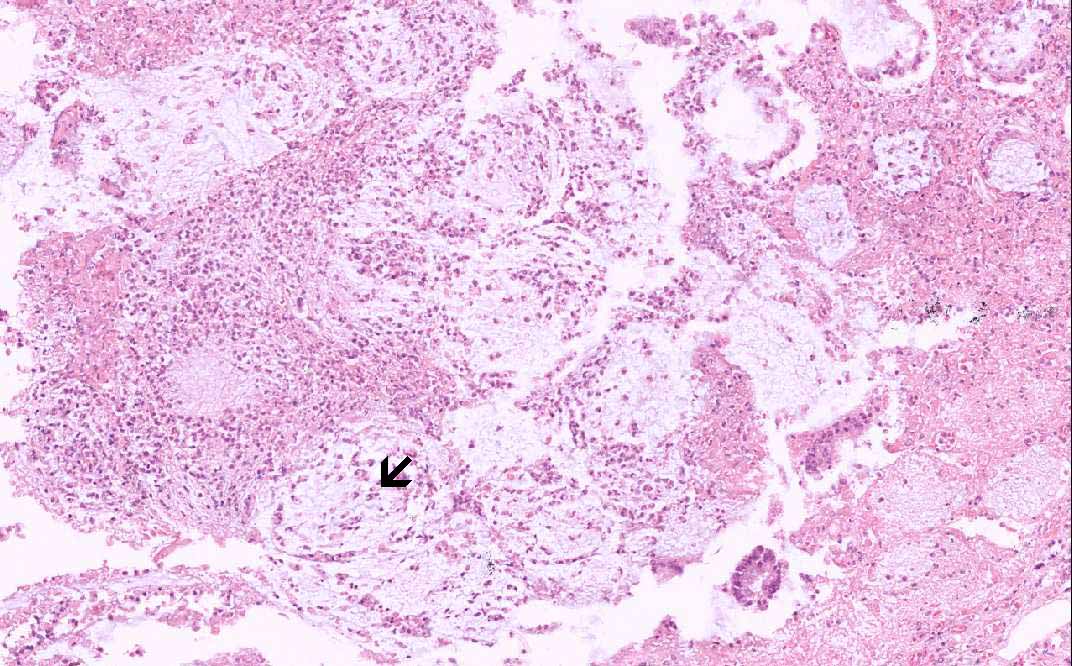
Hematoxylin & eosin |
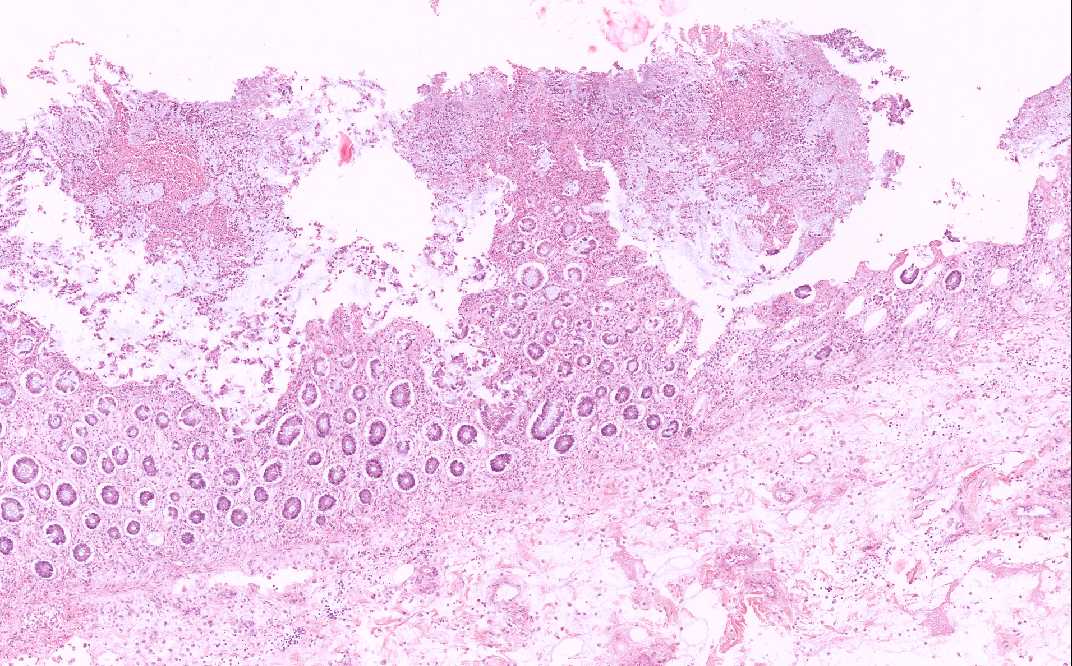
Area 1: The mushroom-like or volcano-like structures are well illustrated here. The overlying inflammatory substance is composed of neutrophils, karyorrhectic debris, and mucin. |
|
Hematoxylin & eosin |
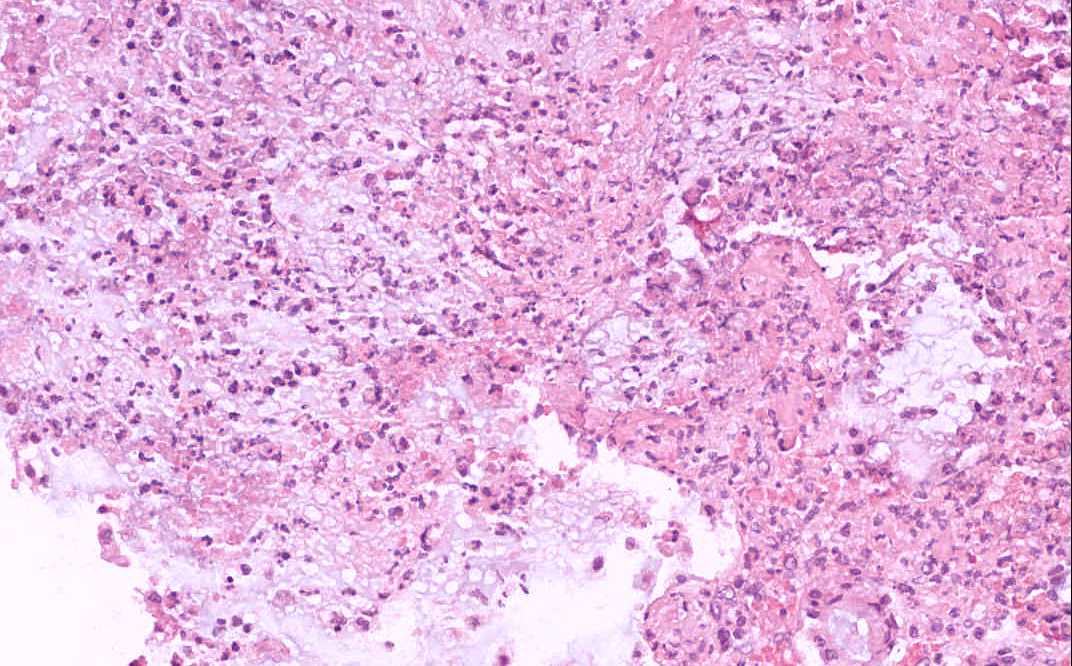
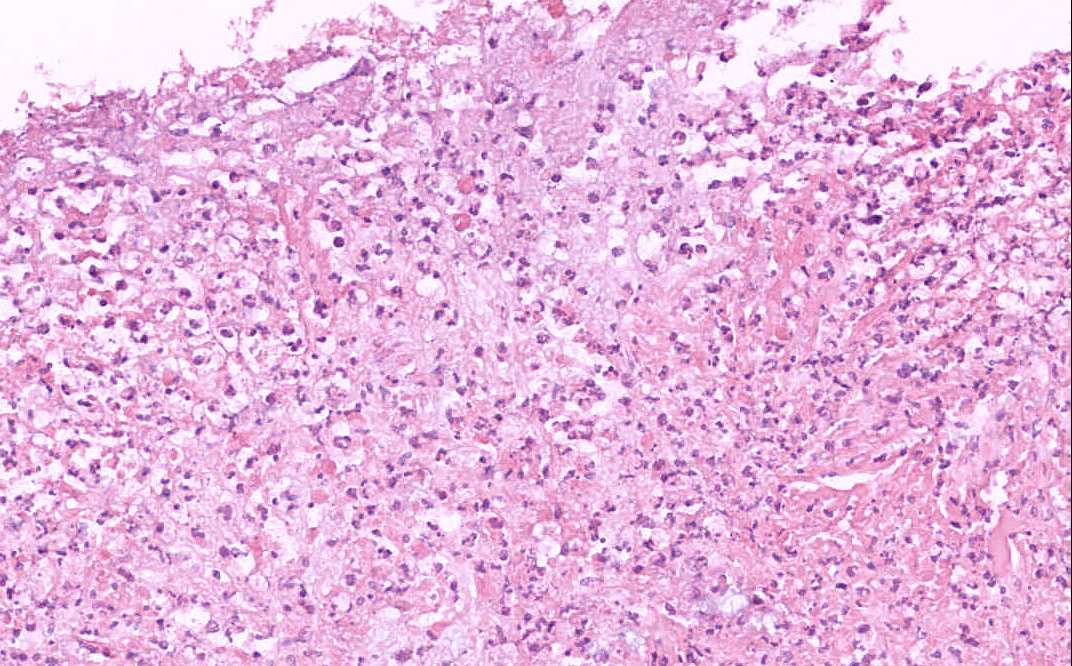
Area 2: Note that the inflammatory necrotic debris has form a pseudomembrane. |
|
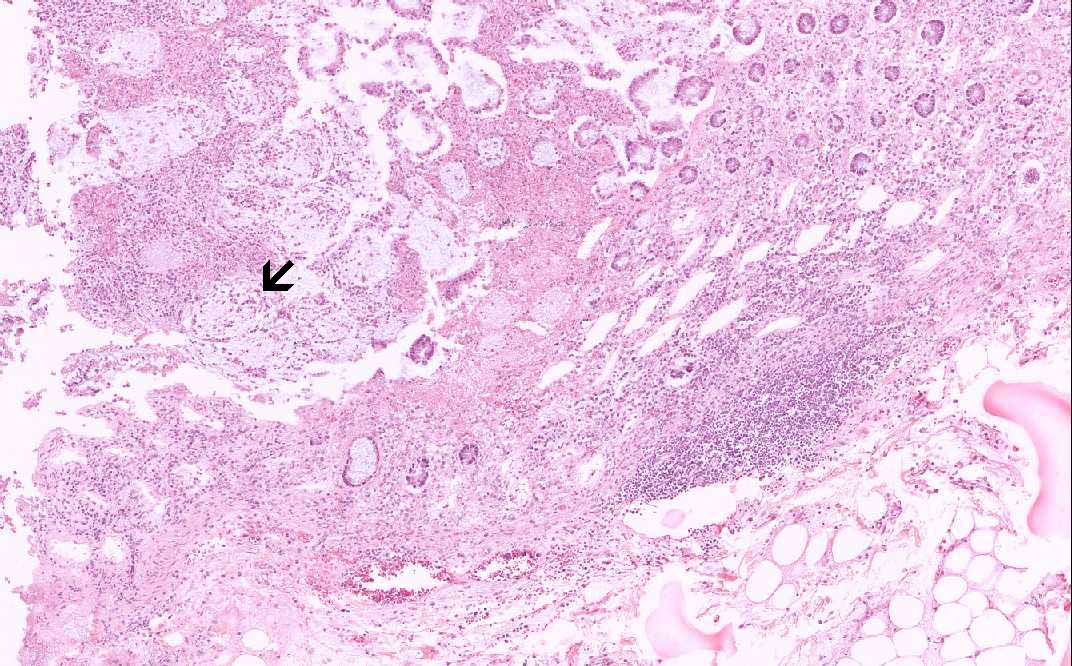
Hematoxylin & eosin |
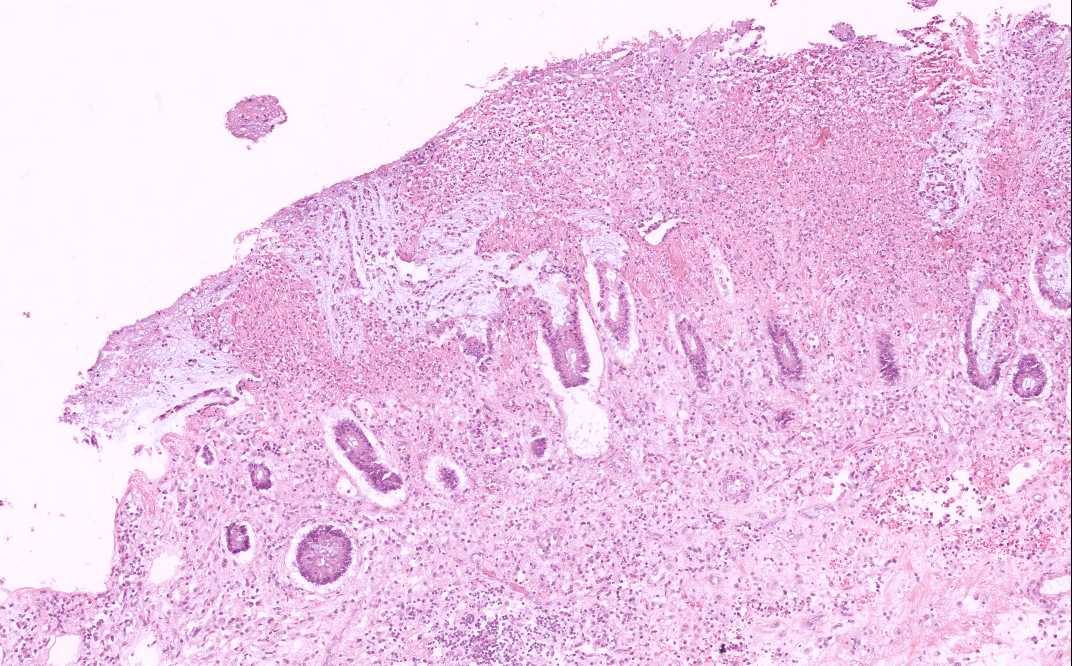
Area 3: Note the interesting linear arrangement of the inflammatory cells and the mucin (arrow). |
|
History: This slide was taken from the archive and the history was uncertain. This type of lesion, however, can mimic a variety of clinical conditions and it is often, but not always, a result of antibiotic therapy. Most of the time symptoms develop during therapy delayed development of this condition may happen. Gross examination of the specimen usually reveal focal plaque like cream to yellow pseudomembrane on the mucosa surface. These membranes are not tightly adhered and can be easily lifted off.
Histologic Highlights of this Case:
Comment: Pseudomembranous colitis is typically caused by the administration of any antibiotics that favor the growth of C. difficile. |
Original slide is contributed by Fred R Dee MD, Department of Pathology, University of of Iowa (Iowa Image Collection).