Case No.: D-003
Diagnosis: Odontogenic keratocyst, central or intraosseous (keratocystic odontogenic tumor)
Organ: Mandible
Last Updated: 12/21/2010
|
|
|
Panoramic view |
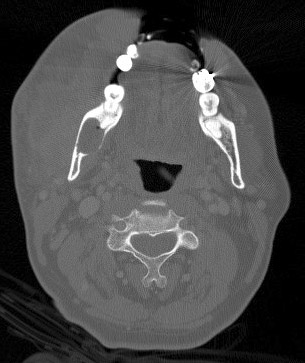
CT scan |
|
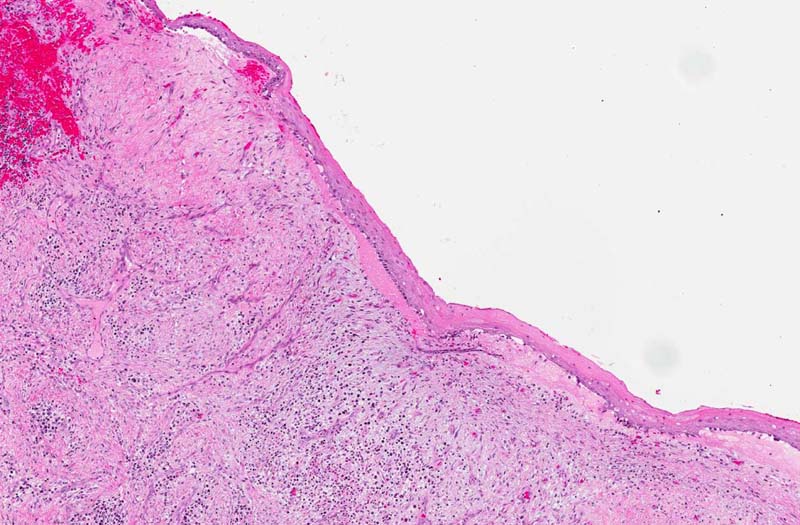
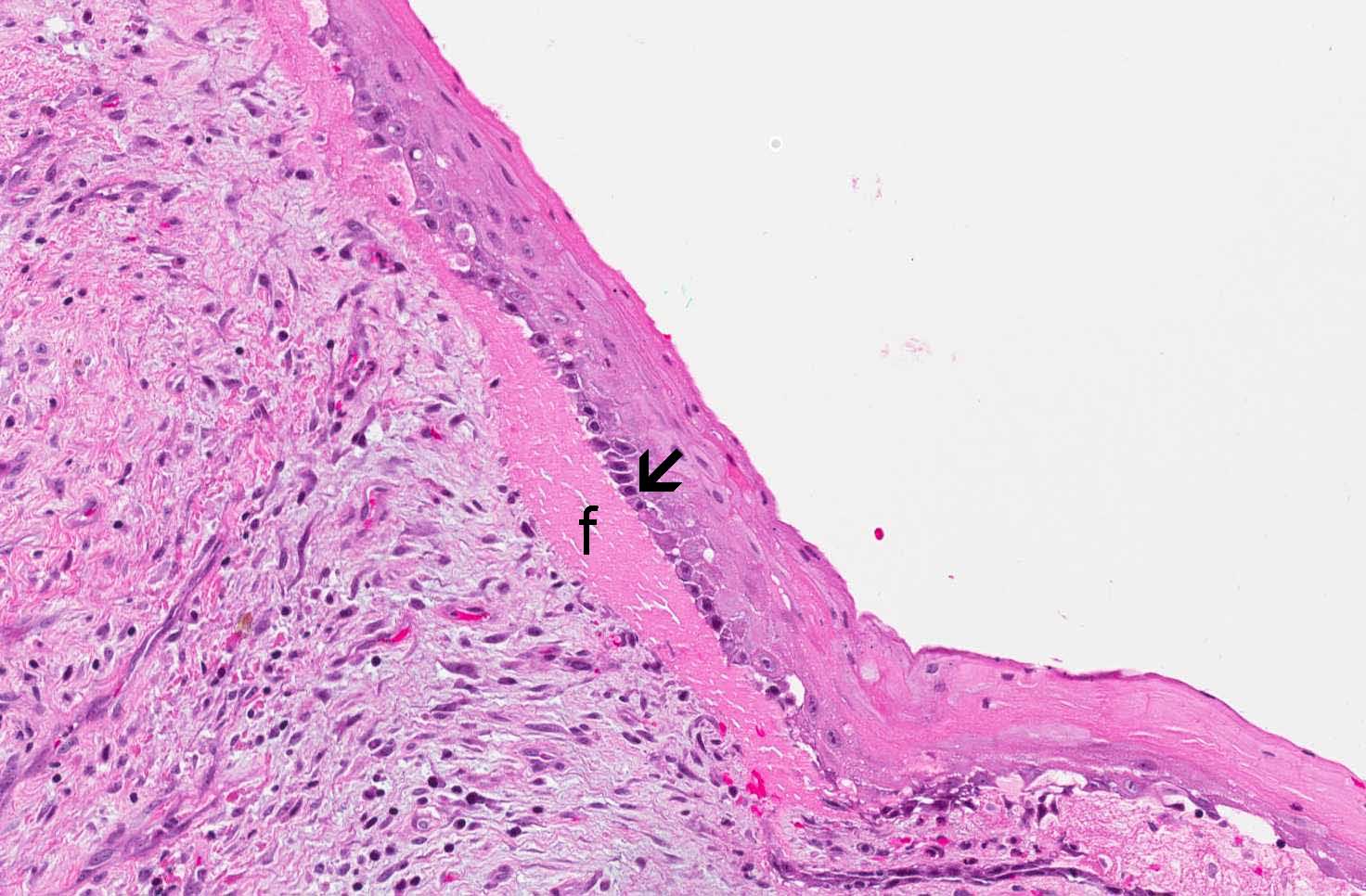
Hematoxylin & eosin |
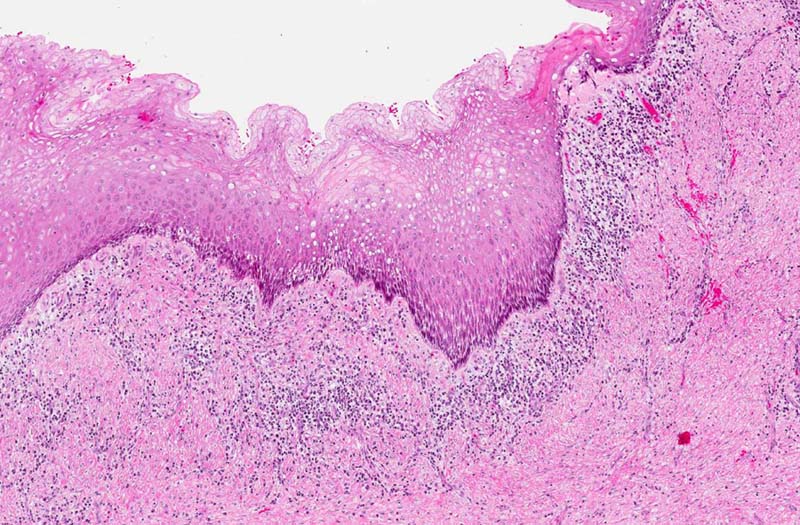
Area 1: Note that there the covering squamous epithelium is thin and free of dysplastic changes. The basal layer is composed of columnar cells with hyperchromatic nuclei, columnar shape, vague palisading arrangement (arrow). A small amount of fibrinous exudate (f) is present in between the squamous epithelium and the underlying stroma. This is not part of the classic features of this type of cyst but rather a result of the inflammation. |
|
Hematoxylin & eosin |
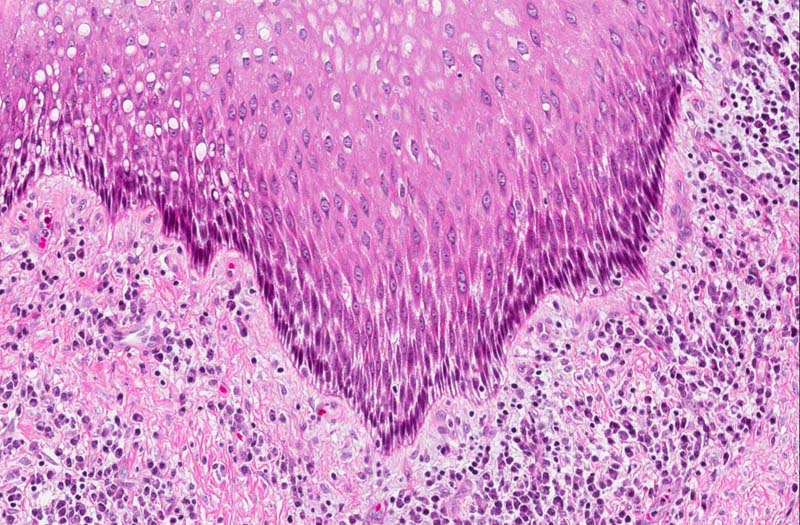
Area 2: In this area, there is thickening of the epidermis. At the same time, this area is also tangentially sectioned which lead to elongation of the nuclei and cells. Note that the degree of chronic inflammatory cell infiltration is more intense in comparison from that of area 1. |
|
Hematoxylin & eosin |
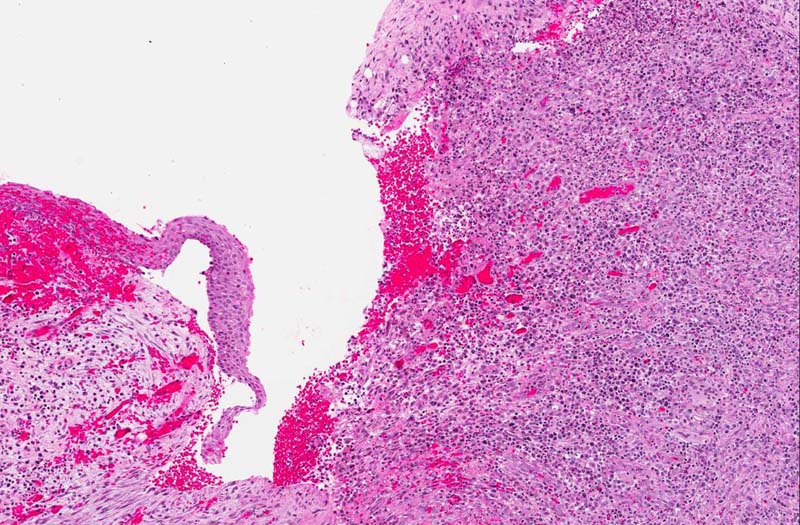
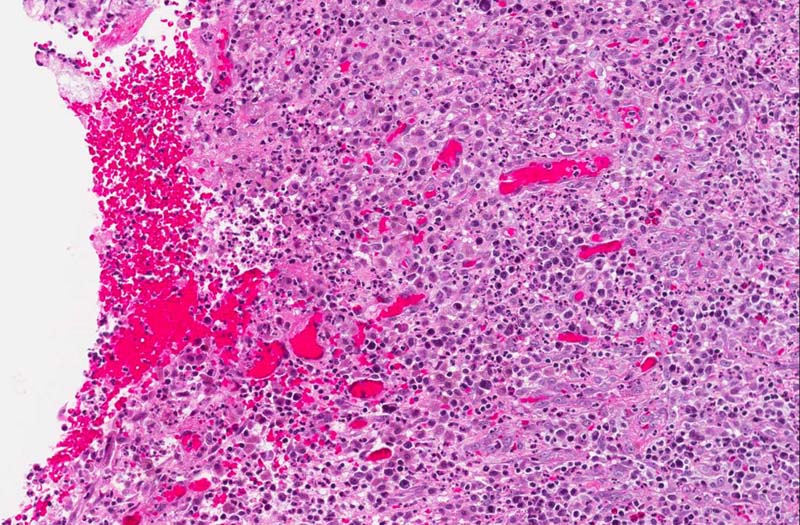
Area 3: The ulcerated area is lined by a mixture of chronic inflammatory cells including lymphocytes and plasma cells. Also present is formation of new blood vessels. |
|
History: The patient was a 49 year-old man who presented with right facial swelling and pain in his jaw, 10 day history of right facial edema, and inability to open his mouth. He was treated with drainage and antibiotics. On further studies, there was a radiolucent lesion at the angle of the mandible suggestive of a cystic lesion. Surgical treatment included incision and drainage of abscess and biopsy of the mandibular cyst which yielded the current specimen.
Imaging:
Histologic Highlights of this Case:
Further Information:
|
Original slide is contributed by Dr. Kar-Ming Fung, University of Oklahoma Health Sciences Center, Oklahoma, U.S.A.

{kind=link}