Case No.: N-002
Diagnosis: Acute infarction (infarction in early phase).
Organ: Cerebellum
Last Updated: 12/21/2009
|
|
|
Hematoxylin & eosin |
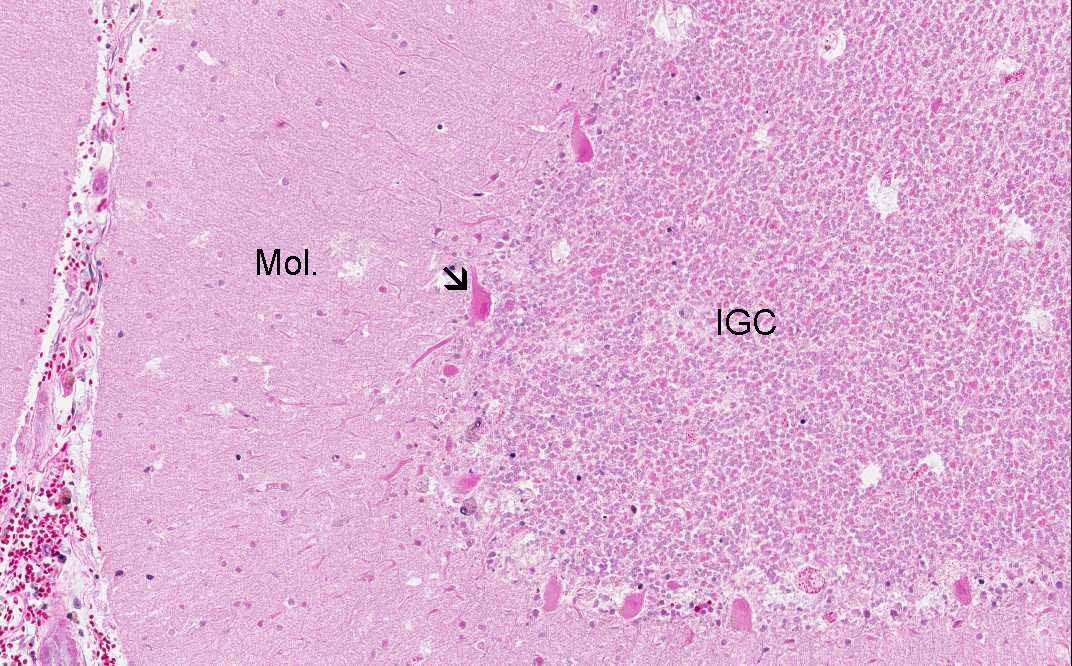
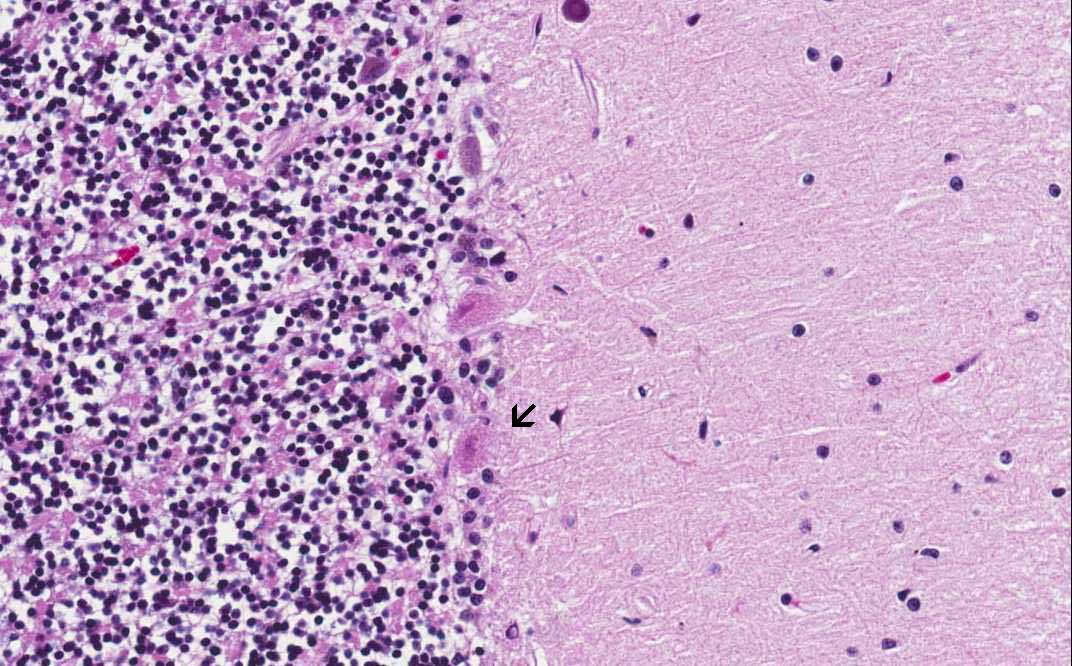
Area 1: The cerebellar gray matter is composed of a paucinuclear molecular layer (Mol.), the Pukinje cells which are composed of large, pyramidal neurons (arrow), and the internal granular cells (IGC). In this image, all the nuclei of these cells are not stained by hematoxylin. On higher magnification, the tissue is dissociating and does not have details. There is no inflammatory cells or macrophages in this lesion. Note that the Purkinje cells are elongated, appears eosinophilic, and does not have details on its nuclear morphology. These are features of necrotic neurons. |
|
Hematoxylin & eosin |
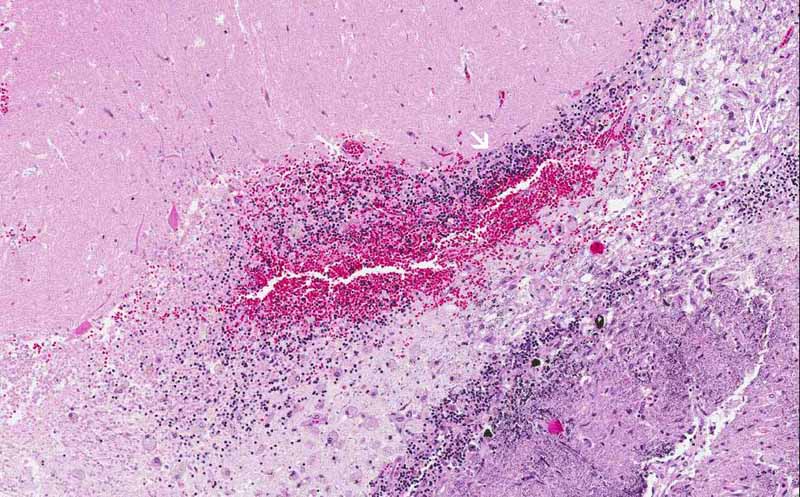
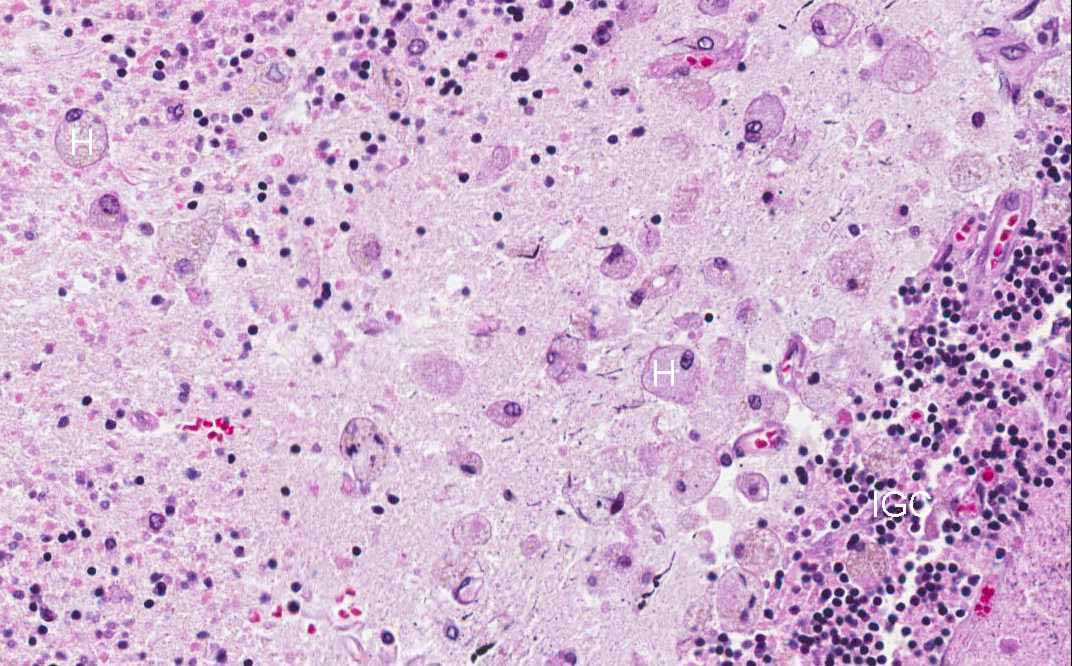
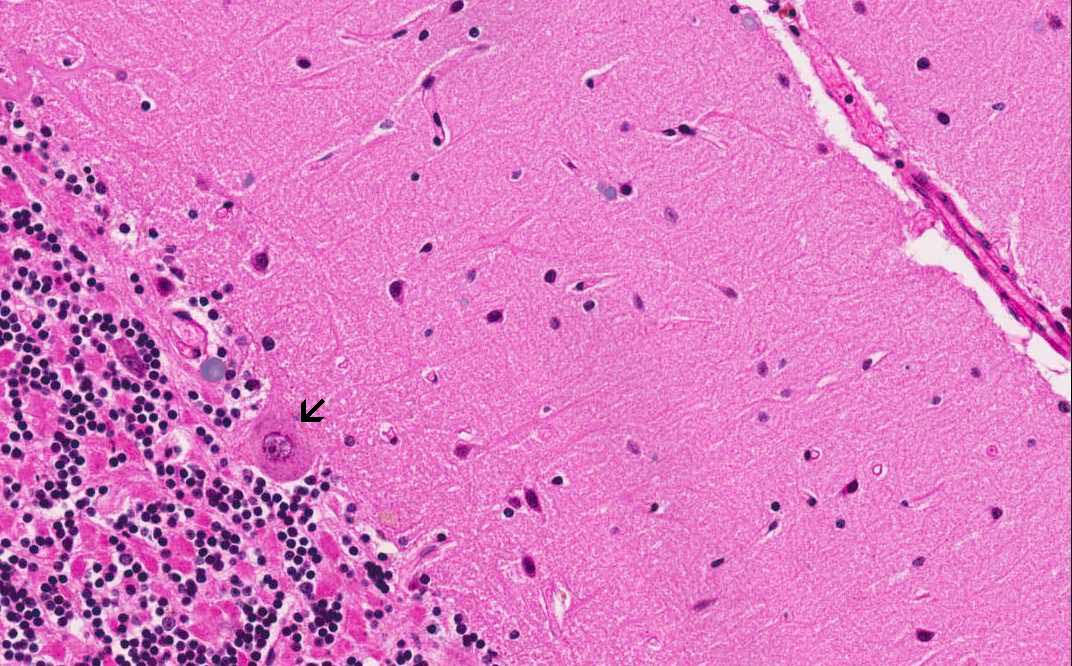
Area 2: At the periphery of the infarct, there is both viable internal granular cells (arrow) with the nuclei well stained by hematoxylin. Foamy histiocytes are noted in the white matter (W). Details of the foamy histiocytes (H) are shown on the panel on the right. Note the viable internal granular cells (IGC). |
|
Hematoxylin & eosin |
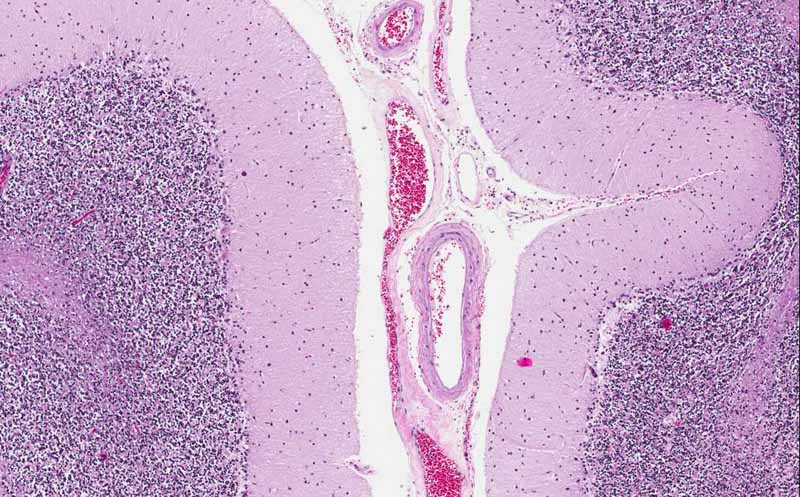
Area 3: In the area remote from the lesion, there is no sign of necrosis. |
|
Hematoxylin & eosin |
Area 3: On high-magnification, however, the Purkinje cells (arrow) does not have normal nuclear details. Compare the nuclear details with the normal Purkinje cells in the panel on the right. The changes here indicate that in addition to the infarction which is a focal process, there is probably a diffuse hypoxic/ischemic event that affects the entire cerebellum. |
|
History: The patient was a 66 year-old man who developed respiratory failure secondary to pneumonia. In the later course of his disease, he also developed sepsis and disseminated intravascular coagulation. In the cerebellum, the patient developed multiple infarcts that measures up to 1.5 cm in greatest dimension.
Gross Pathology: This image is taken from one of the infarcts in the cerebellum. There is an oval, darker lesion (L) involving the cerebellar folia. The cut surface of this area seems to be more irregular than the surround tissue. This area was submitted for microscopic examination and yielded the current slide. There are several much smaller dark areas (arrows).
Histologic Highlights of this Case:
Gross Pathology: The fact that there is tissue disintegration and histiocytic infiltration at the periphery but not the center of the lesion indicate that this sample is obtained at an early stage of resolution and at least about 4 days after the onset of the infarction.
|
Bonus images:
|
Hematoxylin and Eosin Stain |
Luxol Fast Blue and Cresyl Violet Stain |
The two online slides on the left are normal human cerebellum for comparison. Note that the myelin is stained deep blue by Luxol fast blue in the panel on the right. |
Original slide is contributed by Dr. Kar-Ming Fung, University of Oklahoma Health Sciences Center, Oklahoma, U.S.A.