|
History: The patient was a 42 year-old woman who developed knee
pain after a fall about 12 months before. As the pain did not resolve,
she went to see her primary care physician and an osteolytic lesion was
noted in her right fibula upon imaging work up. A biopsy was obtained
followed by the resection with the images being shown here.

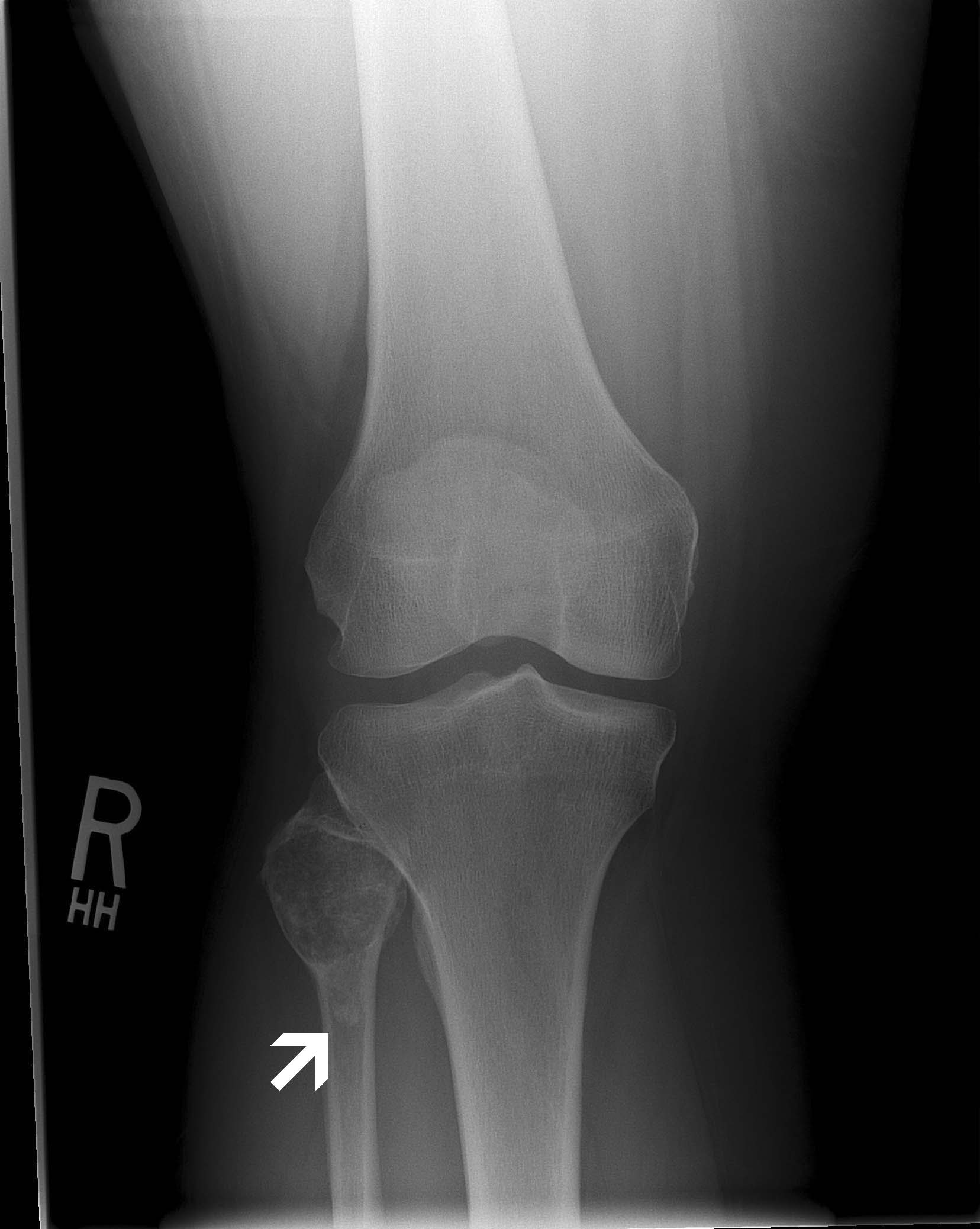
Plain Film:
Note the extension of the osteolytic lesion (arrow) towards the
diaphysis. |
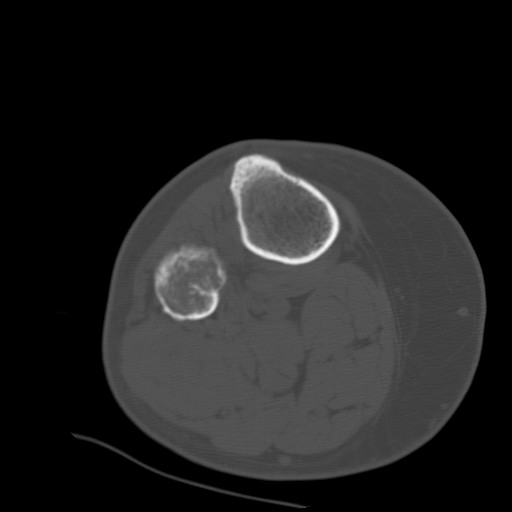
CT:
Note the distruction of the cortex. |
Clinical Perspectives:
-
Chondrosarcoma is the second most common primary bon sarcomas and
represents about one-fourth to one-fifth of all primary bone
sarcomas. It is most commonly seen in the femur, proxima humerus,
scapula and pelvic bones, sternum and ribs.
- It is more common for these tumor to be painful. The diagnosis of
low grade chorndrosarcoma, particularly atypical chondroma/well-diffferentiated
chondrosarcoma of WHO grade I requires correlation of imaging and
histologic findings as histology is often insufficient in separating
enchondroma from well-differentiated chondrosarcoma. Demonstration
of aggressive behavior such as invasion on imaging is needed to
support the diagnosis. A painful low-grade or histologically benign
appearing cartilaginous tumor deserves a thorough search for
evidence of malignancy pointing to a well-differentiated
chondrosarcoma.
- In this particular case there is
extension of the osteolytic lesion (arrow)
towards the diaphysis highly
suggestive of aggressive behavior. On the CT scan, the cortex
overlying the tumor is thickened and blurred which reflects
permeation of haversian and Volkmann's canals with subequent bone
apposition over a long period of time. This is a common feature of a
low-grade chondrosarcoma.
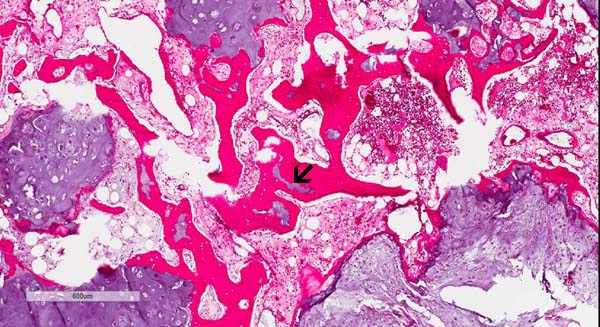
Histologic highlights of this case:
-
A chondrosarcoma is a sarcoma that display phenotypes of
chondrocytes and the matrix formation is uniformly and entirely
chondroid in nature. If neoplastic osteoid formation is present, it
should be classified as an osteosarcoma. Chondroblastic type of
osteosarcoma may contains mostly cartilage and relatively little
neoplastic osteoid therefore search for these neoplastic osteoid
foci is important in making the correct diagnosis.
-
Typically, chondrosarcoma shows mild to moderate levels of
calcification. It should also be noted that the level of
mineralization in chondrosarcoma can vary from tumor to tumor an din
different areas of the same tumor. These calcifications should not
be mistaken as osteoid formation or ossification.
-
The easy way to remember the differences between the three grades of
chondrosarcoma is that the low-grade tumor looks more or less like
cartilage and similar to enchondroma, the intermediate-grade starts
to show definitive increase in cellularity, definitive atypia,
multinucleated tumor cells, and often contains myxoid changes, and
the high-grade tumor has high cellularity, prominent nuclear atypia,
and the presence of mitoses.
-
On the histologic slide, this tumor is composed of a low-grade
neoplastic chondroid of low cellularity. The overall cytologic
features are reminiscent of normal cartilage but they are separated
into numerous lobules separated by thin fibrovascular bands.
These lobules can vary from one to several millimeters in diameter.
The tumor bulge out and disrupted the cortical bone.
-
In another location of the tumor, there is definitive
invasion
of the haversian system. This is an important features for the
diagnosis of chondrosarcoma.
-
Diagnostic wisdom: Demonstration of invasion of the
haversian system and/or the Volkmann's canal are mostly seen
at the periphery where the tumor interface with the bone. However,
this amount of tissue from this location may be limited and rather
fragmented in biopsy material particularly core biopsy. Careful
examination of the available material and correlation with
radiographic findings are the two keys for correct diagnosis.
Molecular Pathology:
References:
-
Amary MF,
Bacsi K, Maggiani F, Damato S, Halai D, Berisha F, Pollock R,
O'Donnell P, Grigoriadis A, Diss T, Eskandarpour M, Presneau N,
Hogendoorn PC, Futreal A, Tirabosco R, Flanagan AM.
IDH1 and IDH2 mutations are frequent events in central
chondrosarcoma and central and periosteal chondromas but not in
other mesenchymal tumours. J Pathol.
2011 Jul;224(3):334-43. Nat Genet. 2011 Nov 6;43(12):1256-61.
-
Somatic mosaic IDH1 and IDH2 mutations are associated with
enchondroma and spindle cell hemangioma in Ollier disease and
Maffucci syndrome.
Pansuriya TC, van Eijk R, d'Adamo P, van Ruler MA, Kuijjer ML,
Oosting J, Cleton-Jansen AM, van Oosterwijk JG, Verbeke SL, Meijer
D, van Wezel T, Nord KH, Sangiorgi L, Toker B, Liegl-Atzwanger B,
San-Julian M, Sciot R, Limaye N, Kindblom LG, Daugaard S, Godfraind
C, Boon LM, Vikkula M, Kurek KC, Szuhai K, French PJ, Bovée JV.
|