
| A 54 year-old Man with
Acute Onset Pain, Delusion, and Rapid Deterioration. August, 2003, Case 308-1. Home Page |
Adeboye O. Osunkoya, M.D. 1, Jiaoti Huang, M.D., Ph.D. 2 Last update: August 31, 2003.
1 Department of Pathology, University of Oklahoma, Oklahoma City, Oklahoma and 2 Department of Pathology, University of Rochester, Rochester, New York
Clinical information: The patient was a 49 year-old man who presented with a 9 cm scrotal mass of unknown duration..
Pathology of the case:
|
|
|
|
|
|
|
| A. | B. | C. | D. | E. | F. |
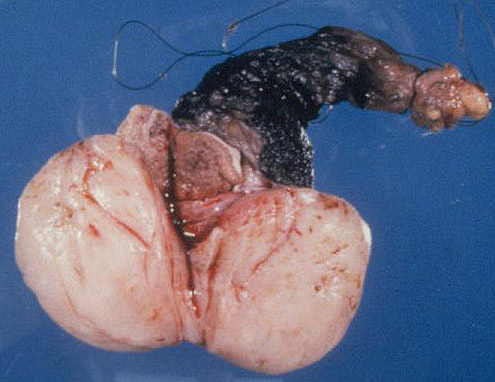
Gross pathology: Panel A shows a 9 cm in diameter round, fleshy to rubbery mass in the scrotal wall. The mass is well circumscribed and does not invade into the surrounding tissue.
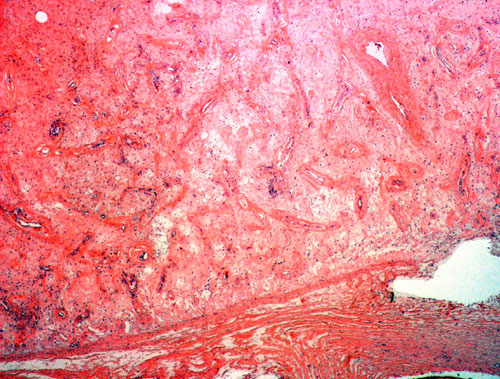
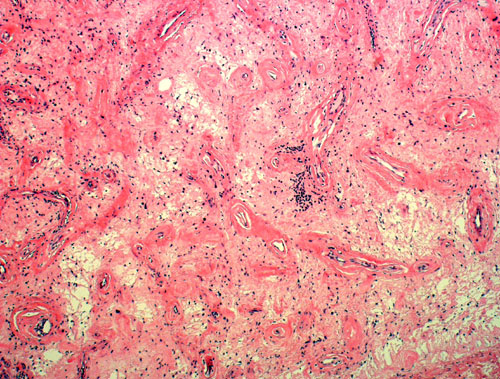
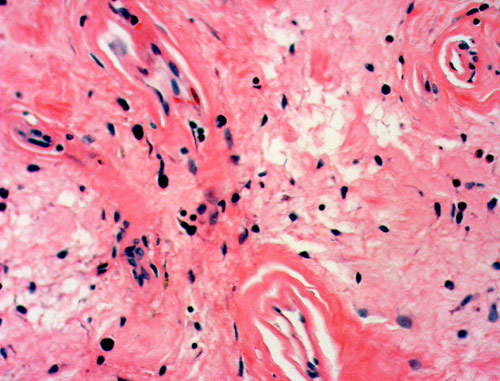
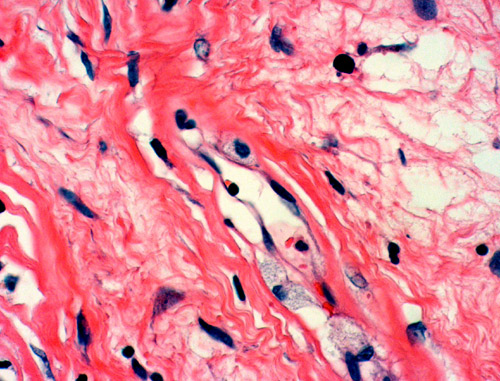
Histopathology: Panel B is taken at the periphery of the tumor where a well circumscribed margin is demonstrated. The tumor has rich vascularity and a hypocellular stroma. However, increased stromal cellularity is present in some areas. Hyalinized blood vessels and a sclerotic to edematous stroma are well demonstrated in Panel C. Also present are a few lymphocytes clustering around blood vessels. The sclerotic stroma with edema and sparse lymphocytic infiltration is demonstrated in Panels D and E. The bland cytologic features are shown in Panel F.
| DIAGNOSIS: Angiomyofibroblastoma of the scrotum. |
Discussion: General Information Pathology Differential diagnosis
General Information
Mesenchymal neoplasms of
the modified genital skin and mucosa are uncommon. Most of these lesions are seen in
females and, collectively, they comprise a family of vulvovaginal soft tissue
tumorsThis family includes the fibroepithelial stromal polyps,
angiomyofibroblastoma, cellular angiofibroma, aggressive
angiomyxoma, vaginocervical myofibroblastoma, vulvar leiomyomatosis, and other smooth
muscle tumors. Uncommon examples of these entities occur in the male
external genitalia.
Angiomyofibroblastoma (AMFB) is a tumor described by Fletcher et al in
1992
1.
The designation “angiomyofibroblastoma” is based on the two integral
components of the tumor: blood vessels and stromal cells. The vascular
component is always prominent and often intimately associated with stromal
cells. Fibroblastic differentiation of the stromal cells is evidenced by the
well-developed Golgi apparatus and prominent rough endoplasmic reticulum by
electron microscopy and by the
collagenous background. Histogenetically it is believed that male AMFB, similar
to its female counterparts
3,
is derived from a perivascular stem cell with a capacity for adipose and
myofibroblastic differentiation probably governed by hormonal, local
microenvironmental, and growth factor/cytokine-related influences
3.
Clinically, AMFB typically involves the vulvar soft tissue of young to middle
aged females,that ranges from 25 to 54
years (mean 36.3 years)
1.
Uncommon male cases of AMFB
2,
3,
4,
5,
6,
7
and AMFB-like tumor
8
have been well documented. The tumor typically presents as a vulvar mass that
usually has its epicenter in the labia majora.
The clinical features may lead to a clinical diagnosis of Bartholin gland cyst
or inguinal hernia. IUncommon sites of these tumors include the female
urethra
9
and fallopian tube
10.
In males, the tumor could present as either a painful or painless scrotal mass,
a hernia or a hydrocele with the typical age ranging from 39 to 88 years (mean 56.6 years)
3.
Macroscopically,
AMFBs range from 0.5 cm to 14 cm in greatest dimension with the majority of them
between 2-8 cm. The lesions are well-circumscribed, round, ovoid, or
lobulated masses with a soft to rubbery consistency. The cut
surface varies from gray-pink to yellowish brown to tan and is of homogeneous texture
with focal myxoid areas. Microscopically, the margin is well
delineated and non-infiltrative. A complete or partial fibrous pseudocapsule of
varying thickness may be present. Some tumors are bordered in part by mature
adipose tissue or smooth muscle. The tumor is characterized by rich
vascularization in a background of collagenous
to edematous stroma with alternating hyper- and hypocellular regions 3.
The stromal background is edematous rather than myxoid. The nature of the
background is supported by negative staining for Alcian blue
stain.
The
stromal cells possess a bland, oval or elongated nuclei and either
scanty, amphophilic cytoplasm with ill-defined margins or eosinophilic, tapered
cytoplasm with better delineated cell borders. Intranuclear inclusions and
longitudinal nuclear grooves are common in the spindle cells. Epithelioid mesenchymal cells with globoid eosinophilic cytoplasm and a single
nucleus or occasional multiple, round nuclei may be present. Mitotic figures
are characteristically rare or absent. The cellularity is quite variable and is
somewhat related to the vascularity. In most cases, the spindled and epitheloid
cells proliferate in a haphazard arrangement. In the more cellular cases,
spindled cells form loosely organizing fascicles. Tumor
cells may aggregate or form masses around blood vessels and those that are close
to blood vessels may have a myoepithelial appearance. The
vascular component of the tumor consists of small to medium-sized, rounded,
curvilinear, non-branching, and thin-walled vessels. Perivascular fibrosis or
sclerosis is a feature detected to some degree in all cases
11.
Mature adipocytes can be sparsely scattered within the neoplasm and, in
rare cases, adipose cells predominate; such tumors have been classified as the
“lipomatous” variant of angiomyofibroblastoma
8
by some investigators. Strong and diffuse immunoreactivity for both desmin and vimentin
is demonstrated in practically all cases. Only a
minority of cells in some cases show positive immunoreactivity for either
smooth muscle actin or pan-muscle actin
1,
12,
13,
14
,
15.
Tumor cells are negative for S-100 protein, cytokeratin, collagen type IV, CD 68
and myoglobin
16.
The few cases examined ultrastructurally have shown fibroblastic features in
most cells, with a minority showing myofibroblastic differentiation
1,
12,
14.
Differential diagnosis
The most important differential diagnosis is aggressive angiomyxoma, first described by Steeper and Rosai 17 in 1983. Although rare examples have been subsequently reported in males 18, 19, 20, the vast majority of these tumors occur in women of reproductive age. Interestingly, rare tumors with a composite morphology of both AMFB and aggressive angiomyxoma have beem descrobed 21. The demographic and histopathologic features of aggressive angiomyxoma and AMFB are compared in the following table:
| Aggressive angiomyxoma | Angiomyofibroblastoma | |
| General: | ||
| Behavior | Locally aggressive, 50% recurrence, does not metastasize. | Superficial, non-infiltrating tumor. No recurrence. |
| Age | 20-50 year-old. | 20-50 year-old. |
| Sex | Women are usually affected although cases in man has also been reported | Mostly seen in women and rarely in man. |
| Location | Pelvic and other perineal locations. (vulva and vagina in women) | Vulva and scrotum. |
|
Size |
3-60 cm | 2-8 cm |
| Histology: | ||
| Margin | Iinfiltrative | Well circumscribed, non-infiltrative |
| Architecture |
Loose and hypocellular myxoid stroma with evenly distributed monotonous small round, spindle or stellate cells. Mast cells & extravasated red cells in stroma. |
Collagenous to edematous stroma with alternating hyper- and hypocellular regions with spindle to round to plasmacytoid cells. |
| Vessels | Non-arborizing, thin-walled ectactic blood vessels and small thick-walled blood vessels. The blood vessels tend to be larger than those in angiomyofibroblastoma. | Rich
vascularity with thin-walled blood vessels
that tend to be of venular or capillary sized. Perivascular fibrosis is
common. Vascularity
somewhat correlated with stromal cellularity. |
| Cellular condensation | Symmetrical and circumferential condensation of stromal cells around blood vessels. | Cells may aggregate or form masses around blood vessels. Cells around blood vessels may have an myoepithelial appearance. |
| Alcian blue | Alcian blue positive stroma | Alcian blue negative stroma |
In addition to aggressive angiomyxoma, there are a few other entities should also be
distinguished from AMFB. An excellent review of the subject is available
22.
Some of the major differential diagnoses are discussed here.
Cellular angiofibroma shares similarities with AMFB in terms of
age, sex, and location
23.
This lesion typically presents as a small, well circumscribed mass.
In contrast to AMFB, focal extension into surrounding tissue can be seen. The cellular
component is composed of spindle cells arranged in short intersecting fascicles
that are admixed with thick walled hyalinized blood vessels and collagen bundles. Although there is brisk mitosis, pleomorphism and
necrosis are absent. These tumors are reported to be benign, with no local recurrences or metastasis
being described.
Superficial angiomyxoma occurs most commonly in the fourth decade of life. Over half of
the cases occur in the trunk and lower extremities. The rest occurs in the upper
extremities, head and neck region and most of the lesions are under 5 cm
24.
In the genital region, about three quarters of the cases occur in females
25.
Grossly, superficial angiomyxoma can be polypoid. Histologically, it is a myxoid neoplasm with moderately to sparsely
cellular myxoid nodules with delicate, thin walled capillary sized blood
vessels. The stromal cells are spindle to stellate in shape and bland. Mitoses are uncommon.
Scattered inflammatory cells, particularly neutrophils, are always present.
About a third of cases may have an epithelial component such as a keratin filled
cyst and epithelial strands. Although benign, about a third of the tumors may be
locally destructive.
Myxoid liposarcoma has been described in the scrotum
26,
spermatic cord
27,
and the vulva
28.
Identification of the lipoblasts allow separation of myxoid
liposarcoma from AMFB. Finally, a series of myxoid sarcoms including the
myxoid malignant fibrosarcoma, myxoid malignant fibrous histiocytoma, and myxoid
melanoma may resemble AMFB. The presence of high grade nuclear features in these
tumors would argue
against a diagnosis of AMFB.
Reference:
Fletcher
CD, Tsang WY, Fisher C, Lee KC, Chan JK.
Angiomyofibroblastoma of the vulva: a benign neoplasm distinct from
aggressive angiomyxoma. Am J Surg Pathol. 1992; 6:378-382.
Siddiqui
MT, Kovarik P, Chejfec G. Angiomyofibroblastoma
of the spermatic cord. Br J Urol . 1997; 79:475-6.
Laskin
WB, Fetsch JF, Mostofi FK. Angiomyofibroblastoma-like
tumor of the male genital tract: analysis of 11 cases with comparison of
female angiomyofibroblastoma and spindle cell lipoma. Am J Surg Pathol.
1998; 22:6-16
Hlaing
T, Tse G. Angiomyofibroblastoma
of the male perineum: An unusual location for a rare lesion. Int J Surg
Pathol. 2000; 8:79-82.
Ito
M, Yamaoka H, Sano K, Hotchi M.
Angiomyofibroblastoma of the male inguinal region. Arch Pathol Lab Med.
2000;124:1697-81.
Garcia
Mediero JM, Alonso Dorrego JM, Nunez Mora C, et al.
Scrotal invasive angiomyofibroblastoma. First reported case. Arch Esp Urol.
2000; 53:827-9.
Modica
G, Cajozzo M, Sciume C, Lupo F, Pisello F, Li Volsi F, Geraci G.
Scrotal angiomyofibroblastoma. Report of a case. Ann Ital Chir. 2001;
72:361-3.
Shintaku
M, Naitou M, Nakashima Y.
Angiomyofibroblastoma-like tumor (lipomatous variant) of the inguinal region
of a male patient. Pathol Int. 2002; 52:619-22.
Kitamura
H, Miyao N, Sato Y, Matsukawa M, Tsukamoto T, Sato T.
Angiomyofibroblastoma of the female urethra. Int J Urol. 1999; 6:268-70.
Kobayashi
T, Suzuki K, Arai T, Sugimura H.
Angiomyofibroblastoma arising from the fallopian tube. Obstet Gynecol. 1999;
94:833-4.
Nielsen
GP, Young RH.
Mesenchymal tumors and tumor-like lesions of the female genital tract: a
selective review with emphasis on recently described entities. Int J Gynecol
Pathol. 2001; 20:105-27.
Nielsen
GP, Rosenberg AE, Young RH, Dickersin GR, Clement PB, Scully RE.
Angiomyofibroblastoma of the vulva and vagina. Mod Pathol. 1996; 9:284-91.
Ockner
DM, Sayadi H, Swanson PE, Ritter JH, Wick MR.
Genital angiomyofibroblastoma. Comparison with aggressive angiomyxoma and
other myxoid neoplasms of skin and soft tissue. Am J Clin Pathol.
1997;107:36-44.
Hisaoka
M, Kouho H, Aoki T, Daimaru Y, Hashimoto H. Angiomyofibroblastoma
of the vulva: a clinicopathologic study of seven cases. Pathol Int. 1995;
45:487-92.
Horiguchi
H, Matsui-Horiguchi M, Fujiwara M, Kaketa M, Kawano M, Ohtsubo-Shimoyamada
R, Ohse H.
Angiomyofibroblastoma of the vulva:report of a case with
immunohistochemical and molecular analysis. Int J Gynecol Pathol. 2003;
22:277-84.
Bigotti
G, Coli A, Gasbarri A, Castagnola D, Madonna V, Bartolazzi A.
Angiomyofibroblastoma and aggressive angiomyxoma: two benign mesenchymal
neoplasms of the female genital tract. An immunohistochemical study. Pathol
Res Pract. 1999;195:39-44.
Steeper
TA, Rosai J.
Aggressive angiomyxoma of the female pelvis and perineum. Report of nine
cases of a distinctive type of gynecologic soft-tissue neoplasm. Am J Surg
Pathol 1983; 7:463-75.
Tsang
WY, Chan JK, Lee KC, Fisher C, Fletcher CD.
A report of four cases occurring in men. Am J Surg Pathol 1992; 16: 1059-65.
Iezzoni
JC, Fechner RE, Wong LS, Rosai J.
Aggressive angiomyxoma in males. A report of four cases. Am J Clin Pathol
1995;104:391-6.
Clatch
RJ, Drake WK, Gonzalez JG.
Aggressive angiomyxoma in men. A report of two cases associated with
inguinal hernias. Arch Pathol Lab Med 1993;117:911-3.
Granter
SR, Nucci MR, Fletcher CD.
Aggressive angiomyxoma: a reappraisal of its relationship to
angiomyofibroblastoma in a series of 16 cases. Histopathology 1997;30:3-10.
Nucci
MR, Fletcher CD.
Vulvovaginal soft tissue tumors: update and review. Histopathology
2000;36(2):97-108.
Nucci
MR, Granter SR, Fletcher CD. Cellular
angiofibroma: a benign neoplasm distinct from angiomyofibroblastoma and
spindle cell lipoma. Am J Surg Pathol. 1997; 21:636-44.
Allen
PW, Dymock RB, MacCormac LB. Superficial
angiomyxomas with and without epithelial components. Report of 30 tumors in
28 patients. Am J Surg Pathol. 1988; 12:519-30.
Fetsch
JF, Laskin WB, Tavassoli FA. Superficial
angiomyxoma (cutaneous myxoma): a clinicopathologic study of 17 cases
arising in the genital region. Int J Gynecol Pathol. 1997; 16:325-34.
Bauer
JJ, Sesterhenn IA, Costabile RA. Myxoid
liposarcoma of the scrotal wall. J Urol. 1995; 153:1938-9.
McFadden
DW. Myxoid
liposarcoma of the spermatic cord. J Surg Oncol. 1989; 40:132-4.
Brooks
JJ, LiVolsi VA.
Liposarcoma presenting on the vulva. Am J Obstet Gynecol. 1987;
156:73-5.