CK7
EMA
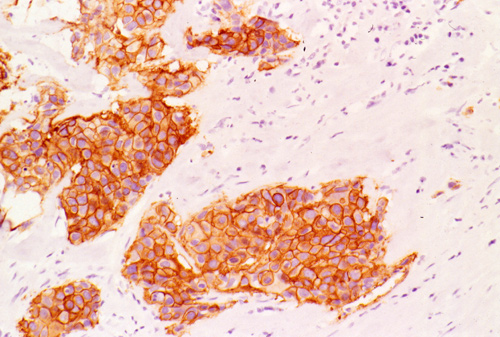
Her2-Neu
| A 50 year-old Man with
a Rapidly Enlarging Parotid Mass. September, 2003, Case 309-3. Home Page |
Cheng Z. Liu, M.D., Ph.D. and Kar-Ming Fung, M.D., Ph.D. Last update: September 30, 2003.
Department of Pathology, University of Oklahoma Health Sciences Center, Oklahoma City, Oklahoma
Clinical information
The patient was a 50 year old man who had a 5 cm parotid mass for a long but uncertain length of time. He complained of recent enlargement of the mass and tenderness. The following photomicrographs were taken from the surgically excised specimen.
Pathology of the case: Click thumbnails to see pictures.
|
|
|
|
|
|
|
| A. | B. | C. | D. | E. | F. |
|
|
|
|
|
|
|
| G. | H. | I. |
J. CK7 |
K. EMA |
L. Her2-Neu |
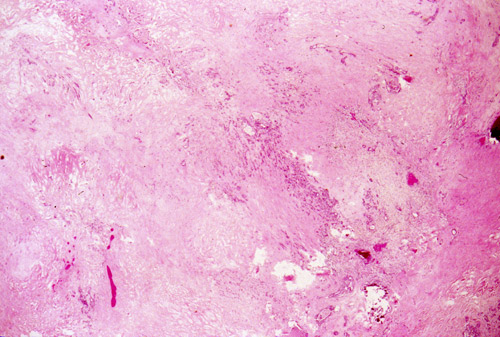
Gross pathology: The tumor mass is 5.5 x 4.5 x 2 cm and appear as a well defined mass but no true capsule. The cut surface is fibrous and with pin-head to small necrotic foci.
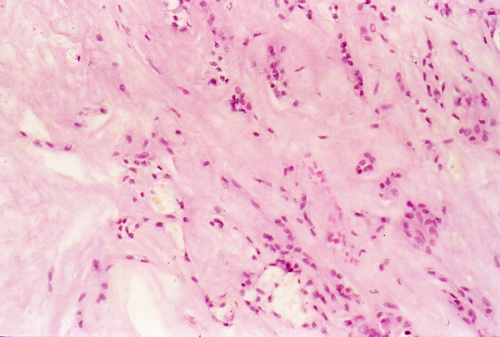
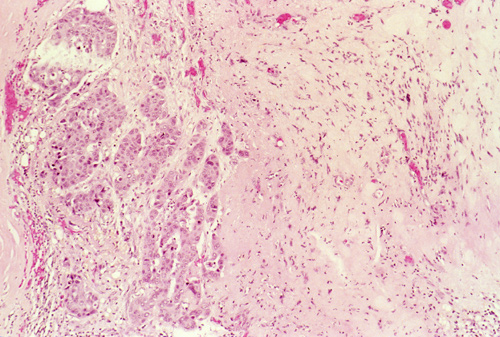
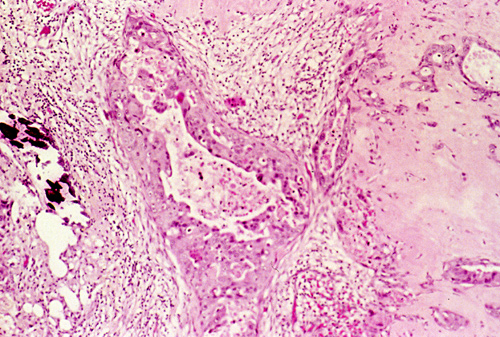
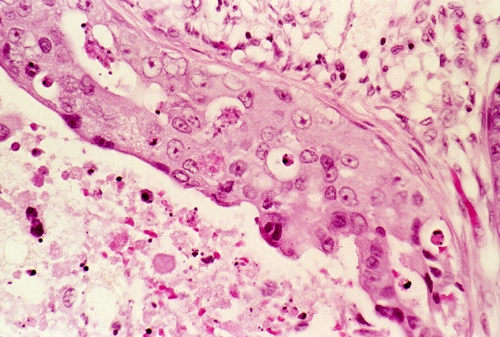
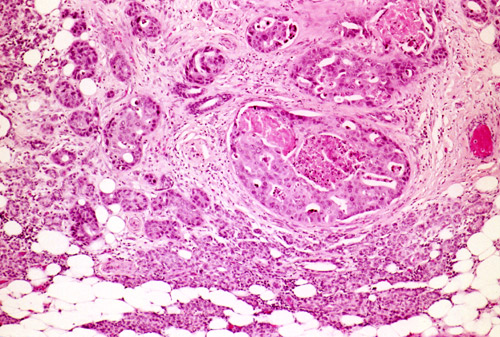
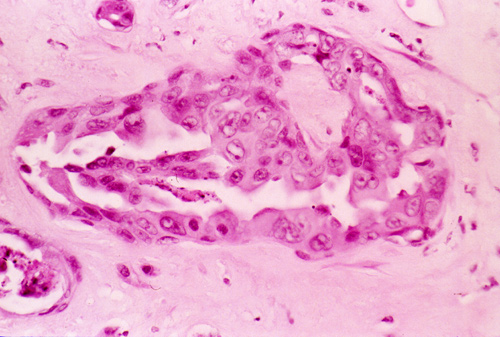
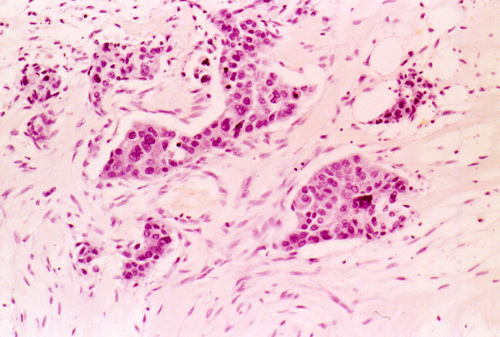
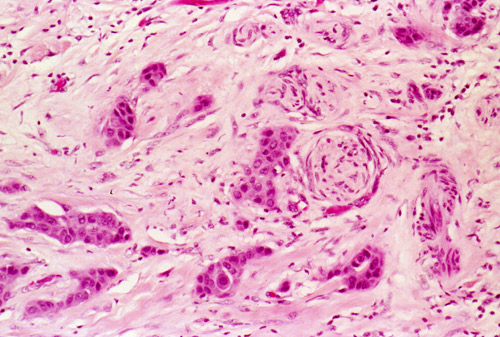
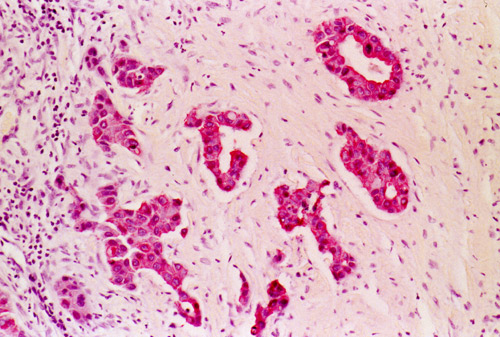
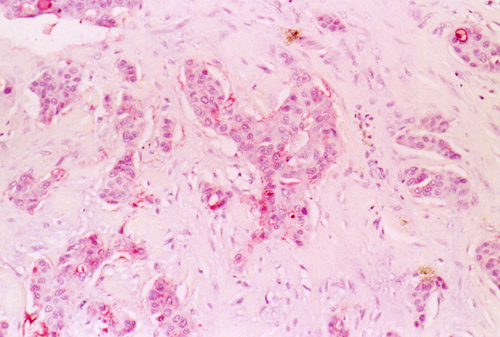
Histopathology: A small portion of the mass has features as illustrated in Panel A, B, and C. These areas have a myxomatous background with strands of bland epithelioid cells (Panel A and B). The large part of the mass is involved by an infiltrative carcinoma. The interface between the myxomatous areas and regions with large and pleomorphic carcinomatous cells is illustrated in Panel C. The carcinomatous cells often form large ductular structures with comedo type necrosis (Panel D and E, Panel E is the higher magnification of Panel D). Ducts with cribiform arrangement of the epithelial cells with and without comedo type necrosis are also common (Panel F and G). In some areas, the invasive carcinoma is accompanied by strong desmoplastic reaction (Panel H). Perineural invasion is present (Panel I) but no definitive vascular tumor emboli are found. The tumor cells are strongly immunoreactive for cytokeratin 7 (Panel J), epithelial membrane antigen (EMA) (Panel K), and Her-2-Neu (Panel L). The carcinomatous cells are not immunoreactive for cytokeratin 20.
| DIAGNOSIS: Salivary duct carcinoma ex pleomorphic adenoma. |
Discussion: General Information Pathology Differential diagnosis
General Information
There are three types of malignant pleomorphic adenoma. The first type is a
benign pleomorphic adenoma that metastasizes as benign pleomorphic adenoma. The
second type is a carcinosarcoma. The third type, and perhaps the most common
type, is carcinoma ex pleomorphic adenoma (CEPA). This condition is a
carcinoma that develops in association with a benign primary or recurrent
pleomorphic adenoma. Although CXPA are uncommon, these lesions account for most
of the reported cases of malignant pleomorphic adenoma. The carcinomatous
component is usually of high histologic grade. These clinically aggressive
lesions often lead to metastasis and a tumor related death.
CEPAs account for 3.6% of all salivary neoplasms and 11.7% of salivary
malignancy 1. It is an aggressive tumor
with high overall mortality. Most of these lesions are found in major salivary
glands. An
asymptomatic mass is the most common symptoms. The tumors range in size
in 1 to 17 cm with a mean of 3.9 cm. Tenderness
and involvement of the facial nerve are seen in some cases. Nearly half of the
patients noticed a painless mass in less than a year
2.
Some
patients may experience rapid expansion of a pre-existing mass. When they occurs
in the major salivary gland, CEPA are 6 times more frequently seen in the
parotid gland than the submandibular gland
2.
As per one large series by Oslen and Lewis, the age range from 34 to 95
years with a mean of 61 years. There is a male predilection and a male:female
ratio of 1.8:1. The ratio of primary to recurrent tumor is about 9:1. Survival
is largely related to clinical staging. While the 5-year survival for stage I
disease is over 80%, the overall 5-year survival is only 37%2.
Malignant
transformation in pleomorphic adenoma occurs most commonly in long-standing
lesions or lesions with multiple local recurrences. The risk increases with the
duration of the tumor. While only 1.6% of malignant transformation occurs in
tumors less than 5 years, the risk for tumors over 15 years is 9.5%
3.
In the current case, the malignant component is a salivary duct carcinoma. This highly aggressive entity bears features that resemble invasive ductal carcinoma of the breast and was first described by Kleinsasser et al. 4 They occur most often in patients over 50 years of age and are four time more common in male than female. The typical symptoms include recent onset and rapid growth of a mass that may be painful and fluctuate in size. The parotid gland, followed by the submandibular gland, is the most common site of origin 5. Salivary duct carcinoma have also been described in sublingual gland and minor salivary gland 6, 7. A small number of them may occur as hybrid carcinoma 8, 9 and, interestingly, salivary duct carcinoma is the most common histologic type in hybrid carcinoma as per the study by Nagao et al. 8
Salivary duct carcinoma ranges from less than 1 cm to over 6 cm in size 10. Some of them may be circumscribed but invasion into the adjacent tissue is common. The cut surface is white to tan, firm, solid, and with variable cystic component. When they arise as CEPA, myxoid and chondroid component of the pleomorphic adenoma may be present.
Histologically, there is a high-grade variant and low-grade variant 11, 12 Some tumors are predominantly infiltrative but there are also predominantly intraductal (>90%) examples. All of these variants closely resemble the invasive ductal carcinoma of breast. In the high-grade variant, the cells are pleomorphic and have comedo type necrosis, intraductal cribiform arrangement of tumor cells, and “Roman bridge” formation. Papillary areas, solid areas, squamous differentiation, and psammoma bodies can all be seen. The tumor cells are large, with large nucleoli and prominent nucleoli. Perineural and intravascular tumor emboli are common. Mitotic figures are abundant. Globet cells are not present, a features that could help to differentiate them from high-grade mucoepidermoid carcinoma. Some may have an oncocytic appearance. The invasive component is typically composed of small clusters of tumor cell aggregates with small lumina or cribiform arrangement. Solid, irregular shaped tumor cell aggregates are also frequent. The stroma is usually dense, fibous, and may be hyalinized. The low-grade variant is less common and has smaller cells with apocrine-type cytoplasmic vacuoles. The nuclei are smaller and have finely dispersed chromatin and small nucleoli. There is only minimal necrosis and mitotic activity. Purely intraductal or minimally invasive salivary duct carcinoma may have an improved prognosis. Mucicarmine and Alcian blue stains are negative.
The
tumor cells are immunoreactive for cytokeratin, epithelial membrane antigen and
carcinoembryonic antigen. No myoepithelial cells can be demonstrated by
immunohistochemistry. The tumor cells express keratin, variably express
epithelial membrane antigen, but do not express S-100 protein and myosin
13,14.
Over
expression of Her-2/neu in salivary gland has recently been documented
15,
16.
Expression of androgen receptor has also been demonstrated
17,
18.
Differential diagnosis
Metastatic
ductal carcinoma from the breast must be ruled out. In situ salivary duct
component is more compatible with a primary salivary duct carcinoma than
metastatic ductal carcinoma of the breast. In addition, salivary duct carcinoma
is rarely positive for estrogen receptor and when they are positive, the
positive cells should comprise no more than a small portion of tumor cell
population
14,
19,
20.
Gross cystic disease fluid protein (GCDFP-15) is expressed in many ductal
carcinoma of the breast. It is also detected by immunohistochemistry in over
three-forth of the salivary duct carcinoma studied and is not helpful in
separating the two entities.
Acinic cell carcinoma may contain a papillary cystic (microcystic)
pattern and other tumor growth configuration such as follicular and solid
arrangement. In addition, acinic cell carcinoma contains a diversified cell type
that include acinar, intercalated duct, vacuolated, clear and glandular cells
Hyalinized fibrous stroma is typical for salivary duct carcinoma but not for
acinic cell carcinoma 10. These lesions
also contain periodic acid Schiff (PAS) positive, diastase-resistant cytoplasmic
granules that are not found in salivary duct carcinoma. In addition, the tumor
cells are much less pleomorphic and lack the high-grade pleomorphism that is
present in high-grade salivary duct carcinoma.
Papillary cystadenocarcinoma lacks the cribiform arrangement of tumor
cells. The cystic and papillary growth pattern, however, may confuse these
lesions with salivary duct carcinoma.
Adenocarcinoma NOS have a wide range of low-, intermediate-, and
high-grade differentiation and demonstrate a rich diversity in growth pattern.
By definition, adenocarcinoma NOS is a diagnosis by exclusion of other
characteristic types of salivary carcinomas. Cribiform arrangement of tumor
cells with comedo necrosis should raise the possibility of salivary duct
carcinoma.
Reference:
Gnepp
DR, Wenig BM. Malignant mixed tumors. In: Ellis G, Anclair P, Gnepp D,
editors. Surgical pathology of the salivary glands. Philadelphia: Saunders;
1991. p 350–368.
Olsen
KD, Lewis JE. Carcinoma
ex pleomorphic adenoma: a clinicopathologic review. Head Neck. 2001;
23:705-12.
Kleinsasser
O, Klein HJ, Hubner G.
Salivary duct carcinoma: a group of salivary gland tumors analogous to
mammary duct carcinoma. Arch Klin Exp Ohren Nasen Kehlkopjheilkd. 1968; 192:
100–105.
Barnes
L, Rao U, Krause J, Contis L, Schwartz A, Scalamogna P. Salivary
duct carcinoma. Part I. A clinicopathologic evaluation and DNA image
analysis of 13 cases with review of the literature.
Oral Surg Oral Med Oral Pathol. 1994; 78:64-73.
Huh
KH, Heo MS, Lee SS, Choi SC. Three
new cases of salivary duct carcinoma in the palate: a radiologic
investigation and review of the literature. Oral Surg Oral Med Oral
Pathol Oral Radiol Endod. 2003; 95:752-60.
Urban
SD, Hall JM, Bentkover SH, Kadish SP. Salivary
duct carcinoma of minor salivary gland origin: report of a case involving
the cavernous sinus. J Oral Maxillofac Surg. 2002; 60:958-62.
Nagao T, Sugano I, Ishida Y, Asoh A, Munakata S, Yamazaki K, Konno A, Iwaya K, Shimizu T, Serizawa H, Ebihara Y. Hybrid carcinomas of the salivary glands: report of nine cases with a clinicopathologic, immunohistochemical, and p53 gene alteration analysis. Mod Pathol. 2002; 15:724-33.
Snyder
ML, Paulino AF.
Hybrid carcinoma of the salivary gland: salivary duct adenocarcinoma adenoid
cystic carcinoma. Histopathology. 1999; 35:380-3.
Ellis
GL, Auclair PL, Gnepp DR, Goode RK. Other malignant epithelial neoplasms. In:
Ellis G, Anclair P, Gnepp D, editors. Surgical pathology of the salivary
glands. Philadelphia: Saunders; 1991. p 471-480.
Delgado
R, Klimstra D, Albores-Saavedra J. Low
grade salivary duct carcinoma. A distinctive variant with a low grade
histology and a predominant intraductal growth pattern. Cancer.
1996; 78:958-67.
Tatemoto
Y, Ohno A, Osaki T. Low
malignant intraductal carcinoma on the hard palate: a variant of salivary
duct carcinoma? Eur J Cancer B Oral Oncol. 1996; 32B:275-7.
Brandwein MS, Jagirdar J, Patil J, Biller H, Kaneko M. Salivary duct carcinoma (cribriform salivary carcinoma of excretory ducts). A clinicopathologic and immunohistochemical study of 12 cases. Cancer. 1990; 65:2307-14..
Barnes
L, Rao U, Contis L, Krause J, Schwartz A, Scalamogna P.
Salivary duct carcinoma. Part II. Immunohistochemical evaluation of 13 cases
for estrogen and progesterone receptors, cathepsin D, and c-erbB-2 protein.
Oral
Surg Oral Med Oral Pathol. 1994; 78:74-80.
Skalova
A, Starek, Kucerova V, Szepe P, Plank L. Salivary
duct carcinoma--a highly aggressive salivary gland tumor with HER-2/neu
oncoprotein overexpression. Pathol Res Pract. 2001; 197:621-6.
Skalova
A, Starek I, Vanecek T, Kucerova V, Plank L, Szepe P, Di Palma S, Leivo I.
Expression of HER-2/neu gene and protein in salivary duct carcinomas of
parotid gland as revealed by fluorescence in-situ hybridization and
immunohistochemistry. Histopathology. 2003; 42:348-56.
Fan
CY, Wang J, Barnes EL. Expression
of androgen receptor and prostatic specific markers in salivary duct
carcinoma: an immunohistochemical analysis of 13 cases and review of the
literature. Am J Surg Pathol. 2000; 24:579-86.
Fan
CY, Melhem MF, Hosal AS, Grandis JR, Barnes EL.
Expression of androgen receptor, epidermal growth factor receptor, and
transforming growth factor alpha in salivary duct carcinoma. Arch
Otolaryngol Head Neck Surg. 2001; 127:1075-9.
Martinez-Barba
E, Cortes-Guardiola JA, Minguela-Puras A, Torroba-Caron A, Mendez-Trujillo
S, Bermejo-Lopez J. Salivary
duct carcinoma: clinicopathological and immunohistochemical studies.
J
Craniomaxillofac Surg. 1997; 25:328-34.
Lewis JE, McKinney BC, Weiland LH, Ferreiro JA, Olsen KD. Salivary duct carcinoma. Clinicopathologic and immunohistochemical review of 26 cases. Cancer. 1996 15; 77:223-30.