Case No.: K-001 Quiz
Diagnosis: Myelolipoma
Organ: Adrenal gland
Last Updated: 08/21/2010
|
|
|
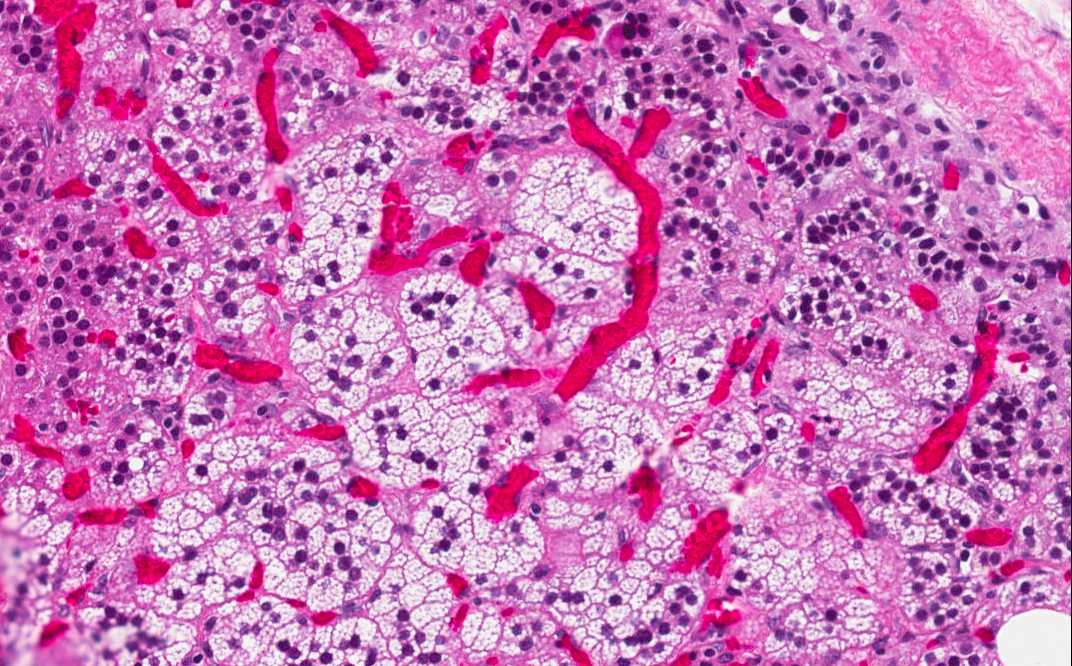
Hematoxylin & eosin |
Area 1: A rim of residual adrenal cortex is present (A) which is separated from the tumor (T). The periadrenal fat (F) is separated from the adrenal gland by a thin layer of fibrous tissue which represent the capsule of the adrenal. Note that the residual cells of the adrenal cortex has many foamy cells due to their high fat content and a rich vascular network which is a common features of many endocrine organs. |
|
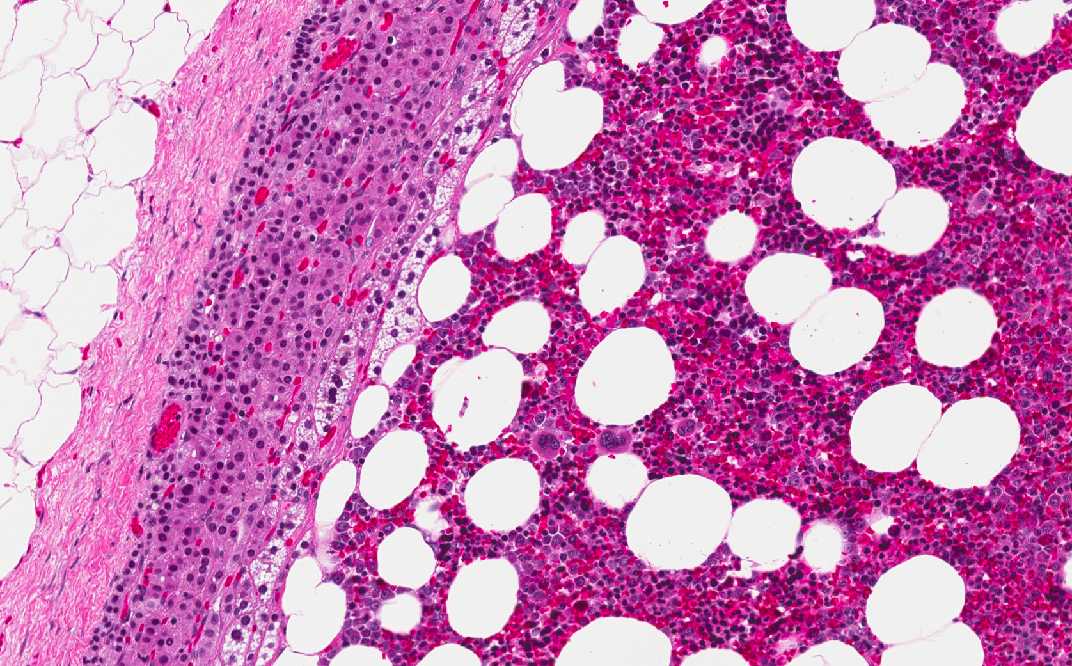
Hematoxylin & eosin |
Area 2: This image is taken from an area where there the tumor has an interface with the residual adrenal cortex. In this area, there are individual adipocytes (A) separated by a backgound of myeloid cells (M). In the high magnification image, you can see a spectrum of myeloid cells in different stages of maturation as well as occasional megakaryocytes. |
|
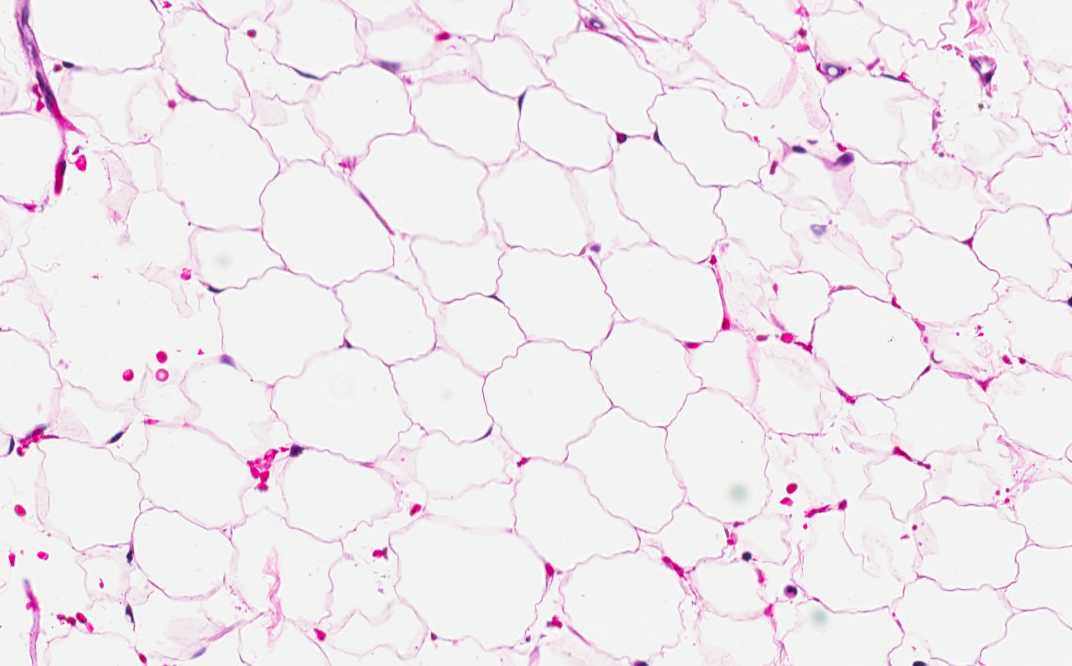
Hematoxylin & eosin |
Area 3: Compare area 2 to the periadrenal adipose tissue, there is no myeloid cells in the peradrenal adipose tissue. |
|
History: The patient was a 50 year old man who was presented to the hospital because of a right kidney mass that is 4.0 cm in diameter that involved the upper pole. A radical nephrectomoy with adrenectomy and the renal tumor was diagnosed to be an clear cell (conventional) renal cell carcinoma, Fuhrman grade II. An incidental 1.2 cm, well demarcated, gray tan nodule was found in the adrenal. The images here are representative of this nodule.
Histologic Highlights of this Case: This section shows a nodule with a thin capsule which represent the capsule of the adrenal gland. There are some crescents of residual adrenal cortical tissue at the periphery of the nodule. The thin capsule represents the capsule of the adrenal gland. The tumor which is composed of a variable mixture of mature adipocytes and mature myeloid cells with trilineage maturation. Note that even though the tumor is well demarcated from the residual adrenal cortex, there is no fibrous septa or capsule between the tumor and the residual adrenal cortex. These cells contains a population identical to mature and active bone marrow. These features are characteristics of adrenal myelolipomas.
Differential Diagnosis:
Comment:
|
Original slide is contributed by Dr. Kar-Ming Fung, University of Oklahoma Health Sciences Center, Oklahoma, U.S.A.