Case No.: N-016
Diagnosis: Colloid cyst with chronic inflammation and histiocytic (macrophage) infiltration
Organ: Brain, 3rd ventricle Quiz
Last Updated: 09/21/2010
|
|
|
Hematoxylin & eosin |
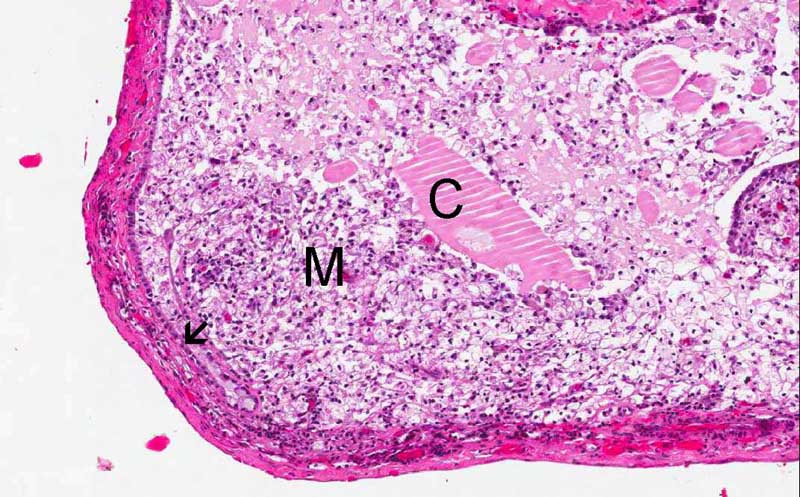
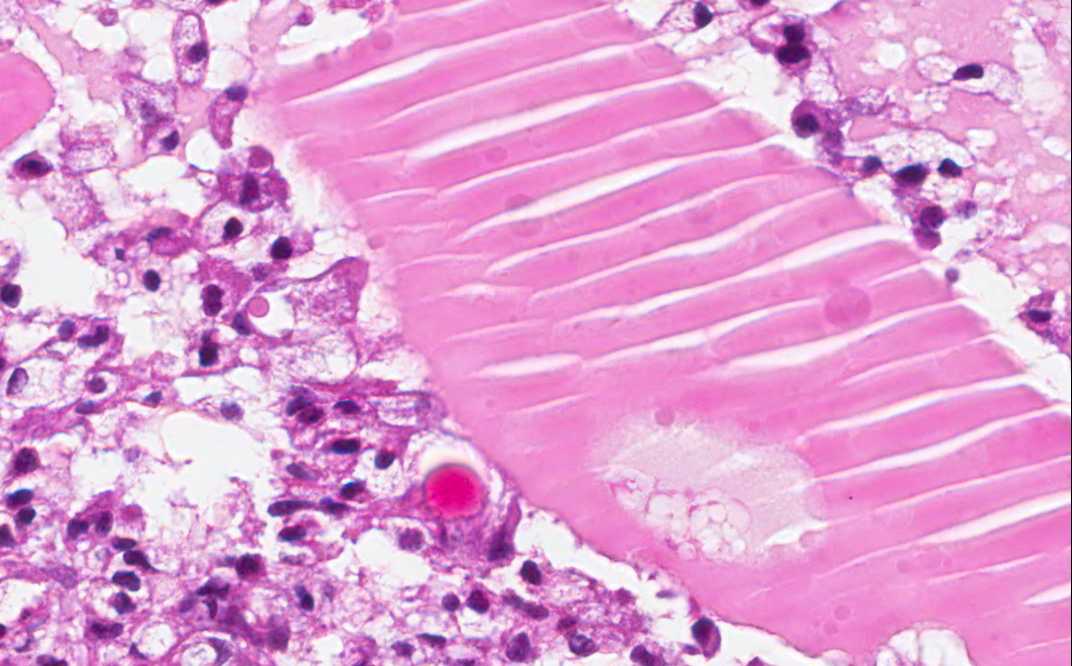
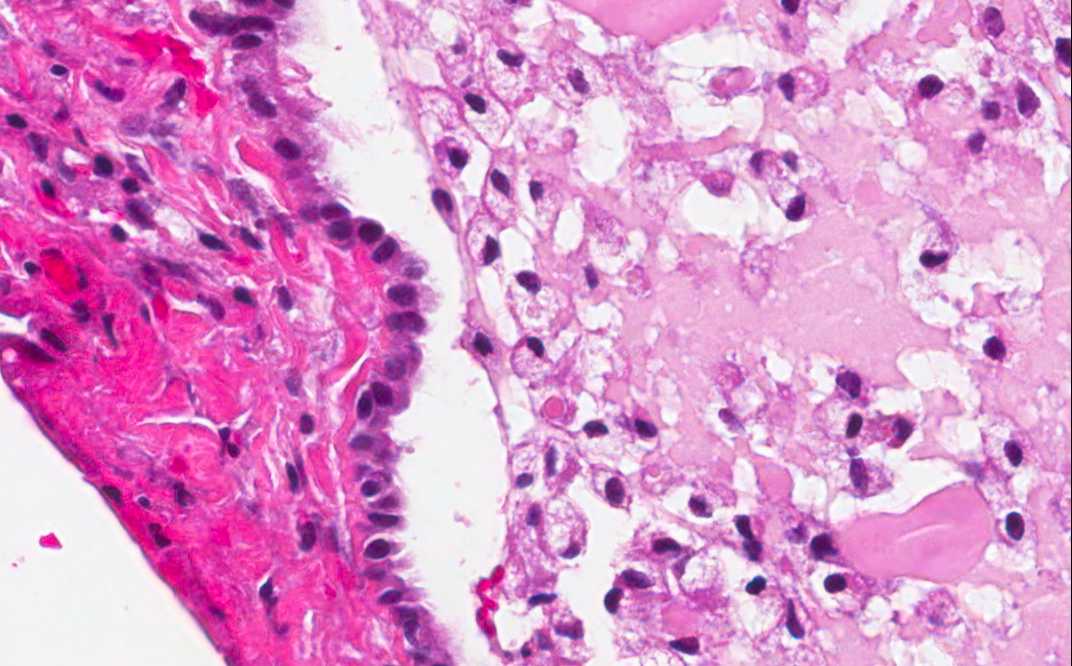
Area 1: The wall of the cyst is composed of a thin fibrous capsule with some chronic inflammatory cell infiltration in some areas. The colloid substance (C) resembles a slab of cut jello with fracture. The cyst is largely filled with foamy histiocytes (M). The lining epithelium (arrow) is a single layer cuboidal epithelium. |
|
Hematoxylin & eosin |
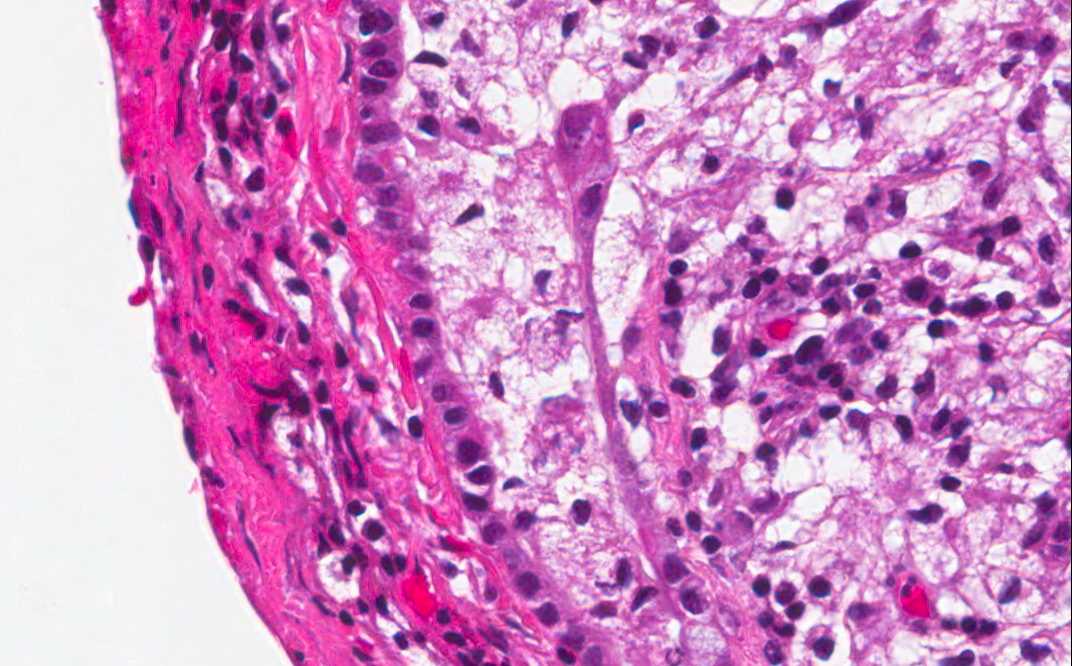
Area 2: The lining epithelium (arrow) is detacthed from the histiocytes. Some of the epithelial cells seem to have cillia. |
|
Hematoxylin & eosin |
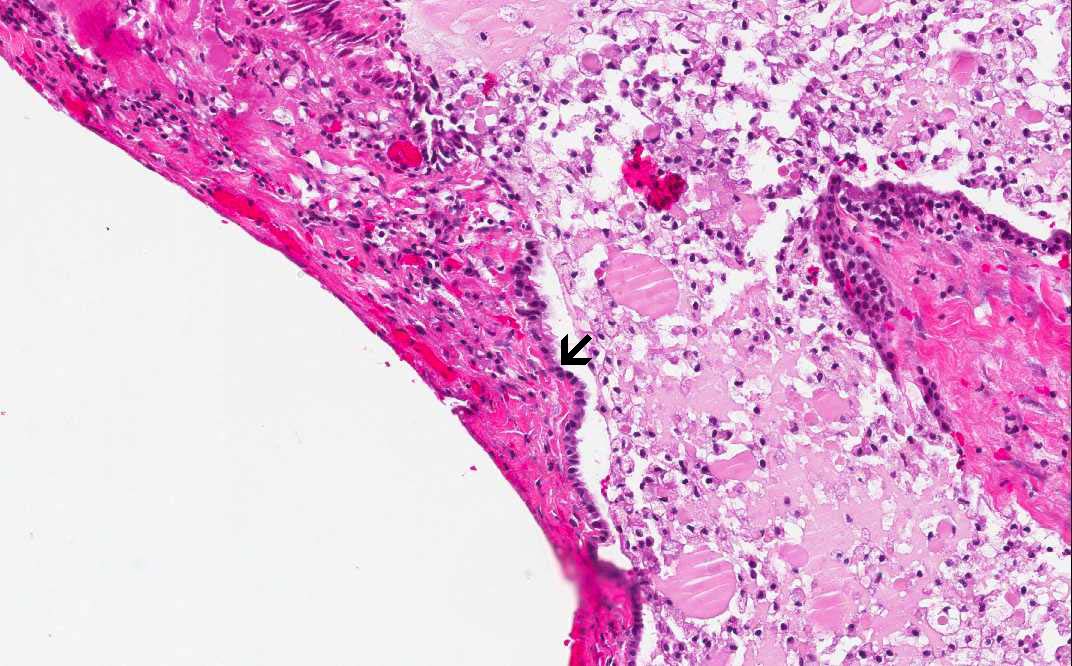
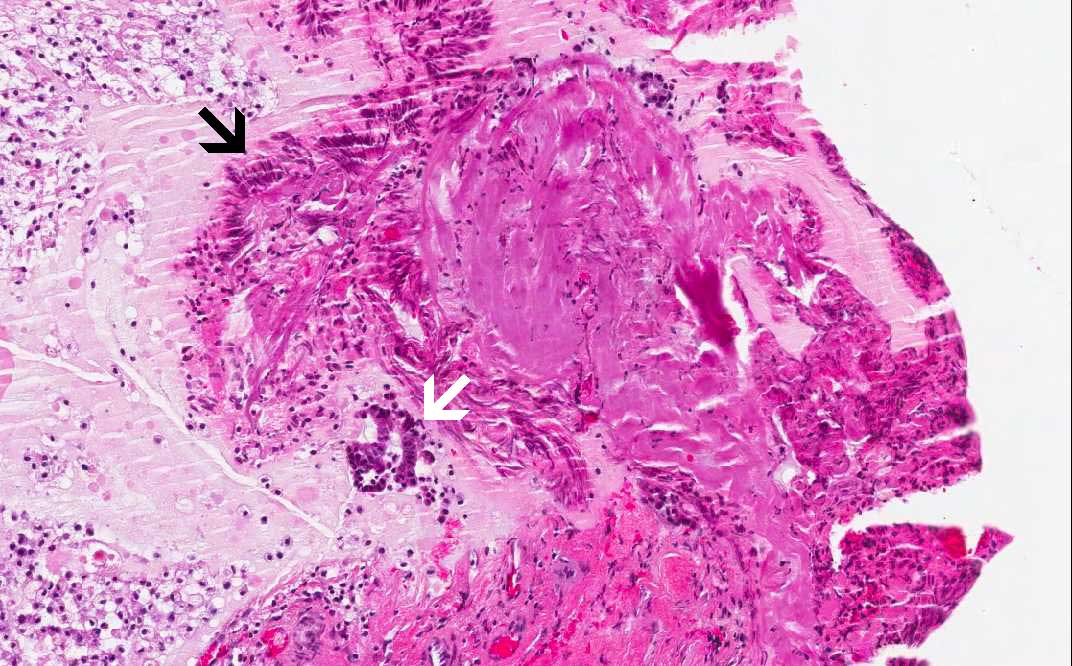
Area 3: The surface of this specimen has sustained cauterization artifacts. The characteristics include loss of details in fibrous tissue and streaming of nuclei (black arrow). Compare these cauterized cells with those free of cauterization artifacts (white arrow). |
History: The patient was a 53
year-old man who presented with a 3 week old history of headache
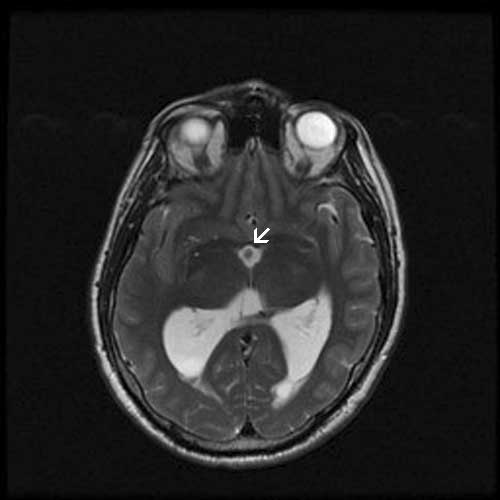
associated with walking and vision changes. Imaging studies demonstrated
prominent dilation of lateral ventricles and a cyst in the third
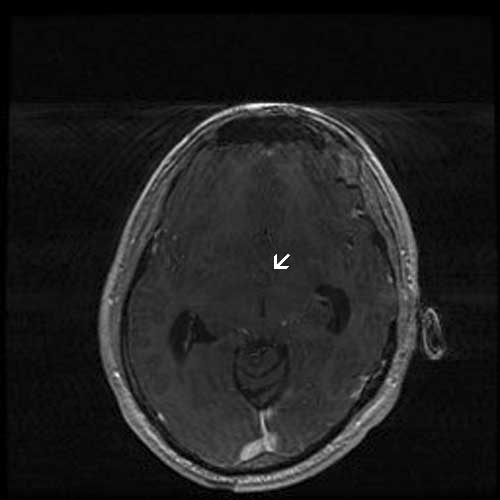
ventricle. On MRI scan, the cyst is 13 x 9 x 9 mm and is located at the
roof of the third ventricle. It has an enhancing mural nodule. The cyst
was removed and generated the specimen here.
Histologic Highlights of this Case:
The lesion is that of an intact cyst
largely filled by foamy histiocytes and some colloid substances. A
thin layer of cublidal to low columnar epithelium is lining the cyst
(Area 1 and 2). There are also mild to moderate chronic inflammatory
cell infiltration in the wall which indicates inflammation. At the
periphery of the lesion has substantial cauterization artifacts
(Area 3).
Most colloid cysts are not heavily
infiltrated by foamy histiocytes as in this one, see bonus images
below.
MRI T1-Contrast
MRI T2
Comment:
Colloid cysts classically locate in the
rostral dorsal aspect of the 3rd ventricle and they are
believed to be congenital in origin. This location is just posterior
to the foramina of Monro, colloid cysts often cause hydrocephalus if
their size is large enough by obstructing the foramin of Monro. For
the same reason, it is well known that change of head position can
be associated with discomfort but this manifestation is rather
uncommon. The location, therefore, is a strong hint for diagnosis.
They are usually seen between the 3rd
and 7th decades.
Grossly, they vary from a few
millimeters to about 3-4 cm in maximum size.
The cyst is usually composed of a thin
collagenous fibrous capsule lined by simple or pseudostratified
layers of cuboidal or columnar (low to high) epithelium with or
without cilia. Goblet cells can be seen.
The colloid content is usually preserved
as a pale eosinophilic, translucent substance resembling a slab of
cut jello. Histiocytic infiltration as illustrated in this case can
be seen but is usually not a prominent feature.
Bonus Images:
|
Hematoxylin & eosin |
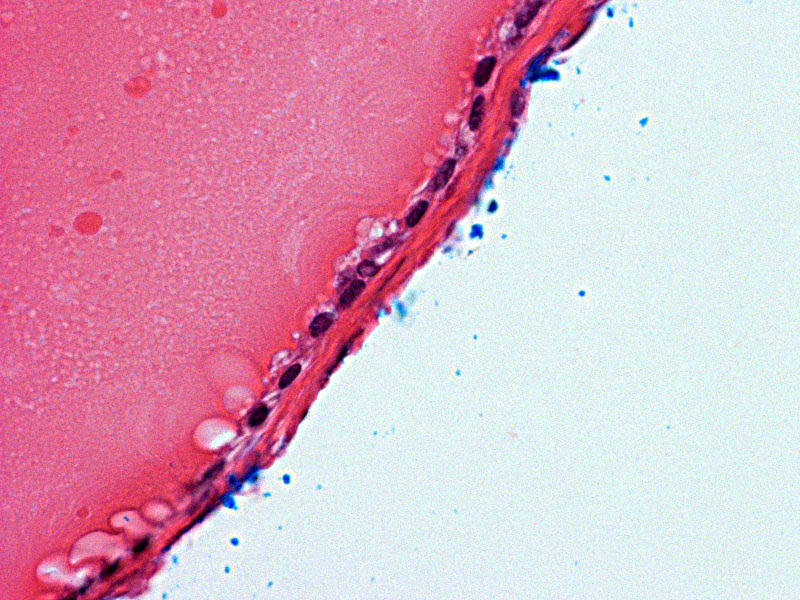
Area 2: This specimen is taken from a different specimen. The colloid cyst is perfectly round, with a paper thin fibrous capsule, lined my a single layer of cuboidal epithelium, and free of histiocytic infiltration. Note that the bright blue substances are surgical inks that we use to mark the margin of specimens. |
Original slide is contributed by Dr. Kar-Ming Fung, University of Oklahoma Health Sciences Center, Oklahoma, U.S.A.