Case No.: N-025 Quiz
Diagnosis: Resolved bilateral occipital lobe infarct
Organ: Brain, cerebral hemispheres
Last Updated: 11/21/2011
|
|
|
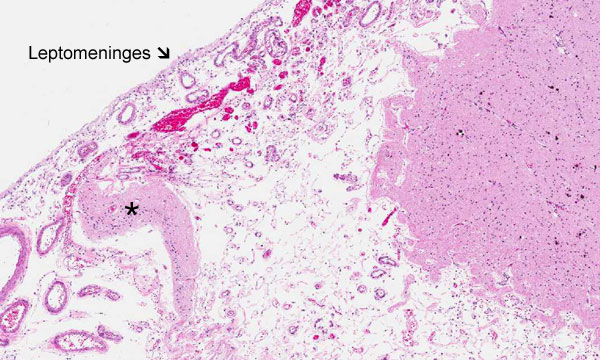
Hematoxylin & eosin |
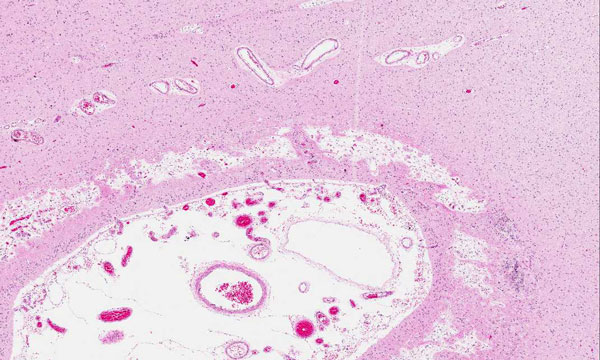
Area 1: Note that small fragments of gliotic brain parenchyma (*) are present under the leptomeninges. The space between the leptomeninges is filled with sparse fibrous tissue originating from the leptomeninges and blood vessels. Scant hemosiderin laden macrophages are also present. |
|
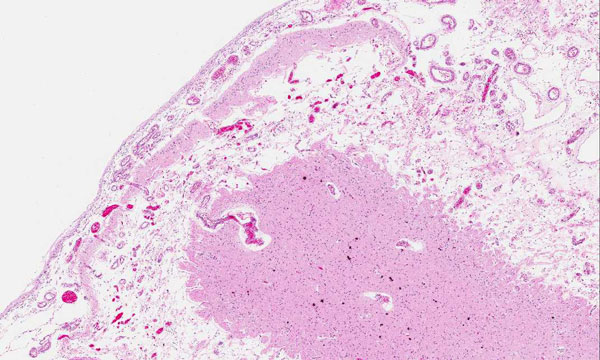
Hematoxylin & eosin |
Area 2: The findings here is very similar to that of Area 1. Note the nodules of dark purple calcifications in the gliotic white matter. |
|
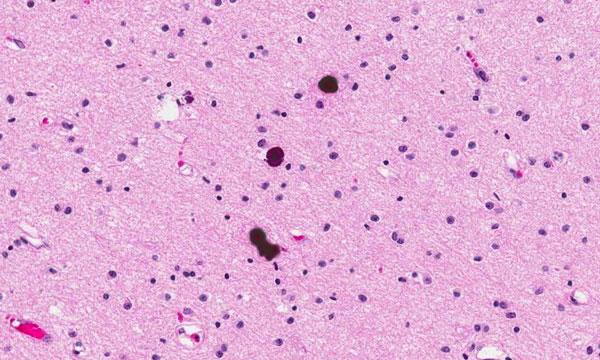
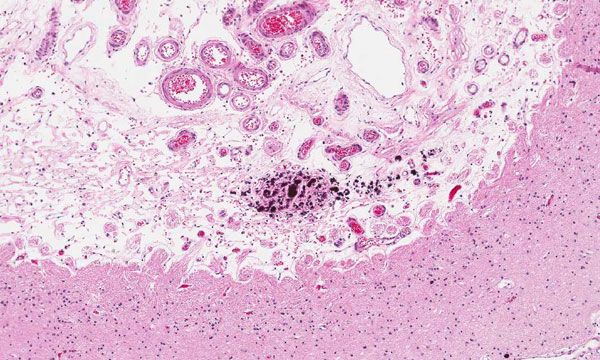
Hematoxylin & eosin |
Area 3: Clusters of dark purple calcifications are also present in the space between the leptomeninges and the gliotic white matter. |
|
Hematoxylin & eosin |
Area 4: Note that the space here is smaller than other areas. This area may be less affected at the time of the insult. |
|
Hematoxylin & eosin |
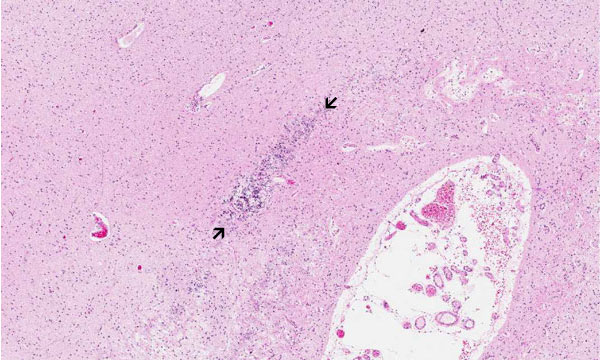
Area 5: This is even less severely affected than Area 4. Note that the streak of calcifications (between arrows) follow the shape of the neuronal layers. |
|
History: The deceased was a 4 year-old boy who has a history of stroke and digital necrosis secondary to Enterococcus faecalis spesis at the age of 6 months. He died of natural causes with autopsy finding including cardiomegaly and dilated right ventricle consistent with right heart failure, chronic ischemic changes in myocardiac muscle, emphysema, chronic bronchitis, and bronchopneumonia.
On autopsy, there was bilateral softening and subpial cyst formation involving the occipital lobes with its distribution consistent with the territory of posterior cerebral artery. The slide being shown here was taken from the occipital lobe.
Histologic Highlights of this Case:
Comment:
|
Original slide is contributed by Dr. Kar-Ming Fung, University of Oklahoma Health Sciences Center, Oklahoma, U.S.A.