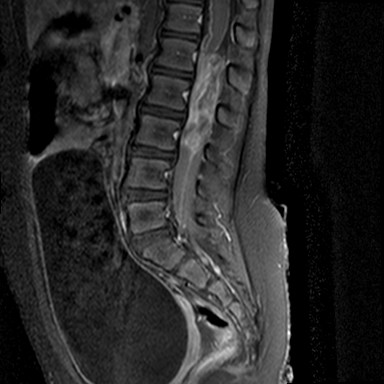
MRI-T1 with contrast
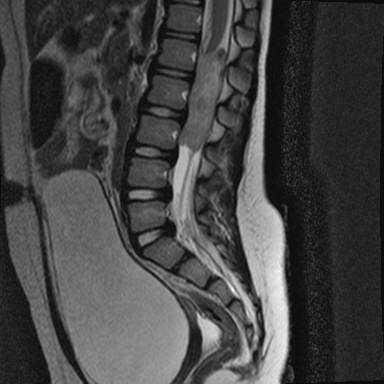
MRI-T2

MRI-T2
Case No.: N-032 Quiz
Diagnosis: Atypical teratoid/rhabdoid tumor (AT/RT)
Organ: Spinal cord L1-L4 and conus medullaris
Last Updated: 12/21/2014
|
MRI-T1 with contrast |
MRI-T2 |
MRI-T2 |
|
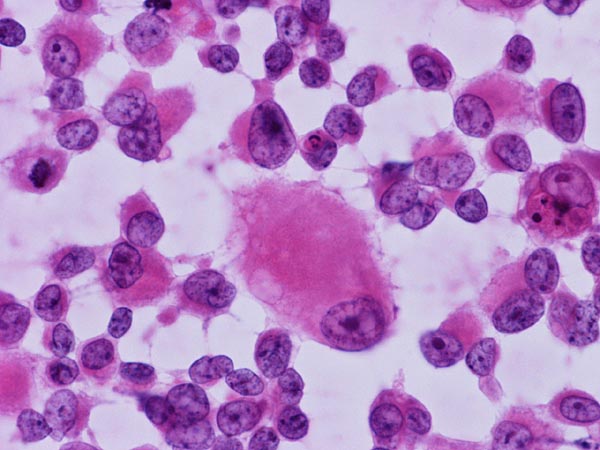
Cytologic squash preparation |
Frozen section |
 Squash preparation |
Squashed cytologic preparation: This smear is essentially diagnostic if you know what you are looking at. It is very important to understand that although rhabdoid cells are part of the features of AT/RT, the number of rhabdoid cells can vary from abundant to scant. Also, the rhabdoid features may not be as dramatic as those being shown in the text book. In this case, if you look at the cells in high magnification then you can see the prominent nucleoli and the moderate amount of eosinophilic cytoplasm. Both features are suggestive of AT/RT. Ependymomal tumors do not usually have these large, prominent nucleoli although they often possess a small but distinct nucleoli. The other differential diagnosis with large nucleoli and is common in pediatric age group is large cell/anaplastic medulloblastoma. However, there is no finding in the brain to suggest dissemination. The large and prominent nuclei may also suggest primary primitive neuroectodermal tumor (PNET) but they are not commonly encountered in PNET. Also, the moderate amount of eosinophilic cytoplasm are not in favor of disseminated medulloblastoma or PNET. These tumor usually contain only a thin rim of cytoplasm. |
|
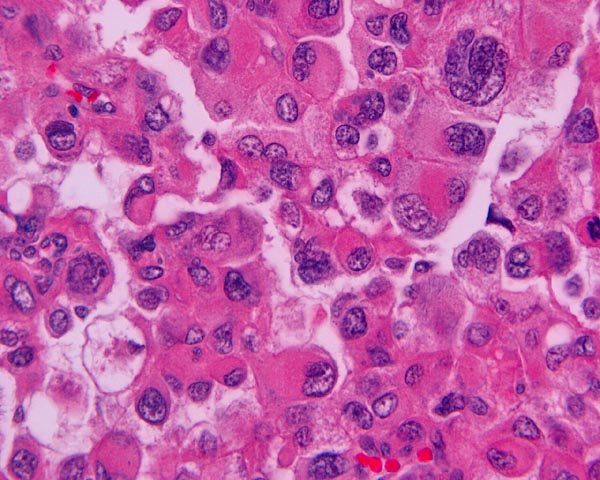
Frozen section |
Frozen section: There is extensive necrosis. In the small piece of viable tumor, you can see some moderately sized cells with enlarged nuclei and prominent nucleoli (white arrow). The nuclei can be eccentrically located and these cells have a moderate amount of cytoplasm. These cells are the rhabdoid cells that you can see in AT/RT. Sometime, the cytoplasmic component is not as prominent and only enlarged nuclei with prominent nucleoli can be found (black arrow). |
|
Intraoperative Consultation:
History: The patient was a 4 year old girl with recent history of difficulty in urination, and paresthesias of left lower extremity and pelvis for two weeks that eventually spread to the right leg. On MRI, there was an intradural mass at the conus medullaris that spanned the L1-L3 area. The lesion filled the spinal cord and was enhancing. The radiographic differential diagnoses include ependymoma.
Intraoperative consultation: There is clearly a large, enhancing, intradural tumor that involves the spinal cord from L1-L3. The conus medullaris is also involved. There seems to be no involvement of the bone. The distended urinary bladder is most likely secondary to involvement of the nerve roots in the lumbar spine.
Differential diagnoses: Based on the radiology and the clinical presentation, several differential diagnoses can be considered with ependymoma with one of the most common one. However, other tumors can give similar pictures. |
 Online Slide/Full Screen/Open with ImageScope |
|
Hematoxylin & eosin |
Area 1: The tumor cells have enlarged nuclei and eosinophilic, prominent nucleoli. However, the cytologic features are not distinctly rhabdoid. |
 EMA |
Epithelial membrane antigen (EMA): In contrast to medulloblastoma and PNET, AT/RT is often positive for EMA. The other common tumor that is often, but not always, positive for EMA in this location and age group is ependymoma. |
 BAF47 |
BAF47: Note that the tumor cells are negative but the entrapped endothelial cells are positive. This indicates that the protein coded by hSNF5/SMARCB1/INI1 is absent. The gene is either deleted or mutated. |
|
Histologic Highlights of this Case:
Immunohistochemistry:
Discussion:
|
Bonus Images from another case:
 |
Rhabdoid cells in cytologic preparation: Note the large cell at the center has a big belly of cytoplasm and at the center is an inclusion body like structure which is rich in vimentin. |
 |
Rhabdoid cells in cytologic preparation: Note the enlarged, eccentrically located nuclei with prominent nucleoli. Note the cytoplasmic inclusion like collection of vimentin rich filament. Under the best optical condition and well prepared slides, these filaments can give a vague fibrillary appearance under the microscope. |
Contributed by Kar-Ming Fung, M.D., Ph.D., University of Oklahoma Health Sciences Center, Oklahoma, U.S.A.



